The California DMV DL 546 form serves as a crucial health questionnaire designed to ensure that drivers meet the necessary medical qualifications to operate a vehicle safely. This form is not intended for commercial licensing requirements, making it specifically relevant for personal drivers. Applicants must provide personal information, including their full name, address, date of birth, and driver license number. The form includes a series of health-related questions that cover a range of potential impairments, from vision and hearing issues to medical conditions like diabetes and heart disease. It is essential for applicants to answer each question honestly, as any “yes” responses may prompt the DMV to contact their physician for further clarification. Additionally, the form must be submitted every two years, emphasizing the importance of ongoing health assessments for drivers. By completing the DL 546, individuals play a vital role in promoting road safety for themselves and others.
*DL546*
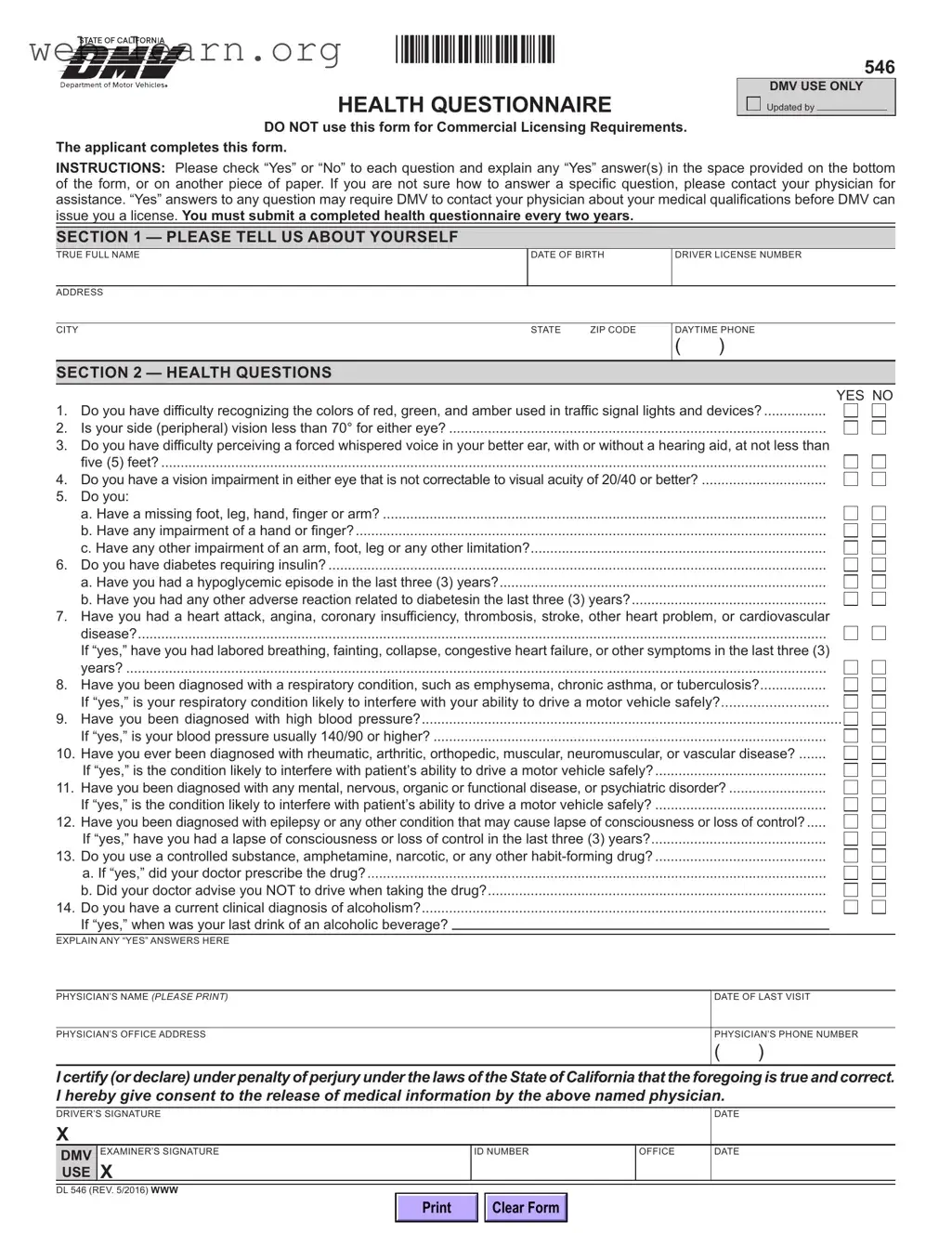
HEALTH QUESTIONNAIRE
546
DMV USE ONLY
Updated by
DO NOT use this form for Commercial Licensing Requirements. The applicant completes this form.
INSTRUCTIONS: Please check “Yes” or “No” to each question and explain any “Yes” answer(s) in the space provided on the bottom of the form, or on another piece of paper. If you are not sure how to answer a specific question, please contact your physician for assistance. “Yes” answers to any question may require DMV to contact your physician about your medical qualifications before DMV can issue you a license. You must submit a completed health questionnaire every two years.
SECTION 1 — PLEASE TELL US ABOUT YOURSELF
TRUE FULL NAME |
DATE OF BIRTH |
DRIVER LICENSE NUMBER |
||
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIP CODE |
DAYTIME PHONE |
|
|
|
|
( |
) |
SECTION 2 — HEALTH QUESTIONS
|
|
|
YES NO |
1. |
Do you have difficulty recognizing the colors of red, green, and amber used in traffic signal lights and devices? |
||
2. |
Is your side (peripheral) vision less than 70° for either eye? |
||
3. |
Do you have difficulty perceiving a forced whispered voice in your better ear, with or without a hearing aid, at not less than |
||
|
five (5) feet? |
||
4. |
Do you have a vision impairment in either eye that is not correctable to visual acuity of 20/40 or better? |
||
5. |
Do you: |
||
|
a. Have a missing foot, leg, hand, finger or arm? |
||
|
b. Have any impairment of a hand or finger? |
||
|
c. Have any other impairment of an arm, foot, leg or any other limitation? |
||
6. |
Do you have diabetes requiring insulin? |
||
|
a. Have you had a hypoglycemic episode in the last three (3) years? |
||
|
b. Have you had any other adverse reaction related to diabetesin the last three (3) years? |
||
7. |
Have you had a heart attack, angina, coronary insufficiency, thrombosis, stroke, other heart problem, or cardiovascular |
||
|
disease? |
||
|
If “yes,” have you had labored breathing, fainting, collapse, congestive heart failure, or other symptoms in the last three (3) |
||
|
years? |
||
8. |
Have you been diagnosed with a respiratory condition, such as emphysema, chronic asthma, or tuberculosis? |
||
|
If “yes,” is your respiratory condition likely to interfere with your ability to drive a motor vehicle safely? |
||
9. |
Have you been diagnosed with high blood pressure? |
||
|
If “yes,” is your blood pressure usually 140/90 or higher? |
||
10. |
Have you ever been diagnosed with rheumatic, arthritic, orthopedic, muscular, neuromuscular, or vascular disease? |
||
|
If “yes,” is the condition likely to interfere with patient’s ability to drive a motor vehicle safely? |
||
11. |
Have you been diagnosed with any mental, nervous, organic or functional disease, or psychiatric disorder? |
||
12. |
If “yes,” is the condition likely to interfere with patient’s ability to drive a motor vehicle safely? |
||
Have you been diagnosed with epilepsy or any other condition that may cause lapse of consciousness or loss of control? |
|||
|
If “yes,” have you had a lapse of consciousness or loss of control in the last three (3) years? |
||
13. |
Do you use a controlled substance, amphetamine, narcotic, or any other |
||
|
a. If “yes,” did your doctor prescribe the drug? |
||
|
b. Did your doctor advise you NOT to drive when taking the drug? |
||
14. |
Do you have a current clinical diagnosis of alcoholism? |
||
|
If “yes,” when was your last drink of an alcoholic beverage? |
|
|
EXPLAIN ANY “YES” ANSWERS HERE
PHYSICIAN’S NAME (PLEASE PRINT) |
DATE OF LAST VISIT |
|
|
|
|
PHYSICIAN’S OFFICE ADDRESS |
PHYSICIAN’S PHONE NUMBER |
|
|
( |
) |
I certify (or declare) under penalty of perjury under the laws of the State of California that the foregoing is true and correct. I hereby give consent to the release of medical information by the above named physician.
DRIVER’S SIGNATURE |
|
|
DATE |
|
X |
EXAMINER’S SIGNATURE |
ID NUMBER |
OFFICE |
DATE |
DMV |
||||
USE |
X |
|
|
|
DL 546 (REV. 5/2016) WWW |
|
|
|
|
|
Clear Form |
|
|
|
| Fact Name | Details |
|---|---|
| Form Purpose | The DL 546 form is a health questionnaire for California driver's license applicants. |
| Commercial Licensing | This form is not to be used for commercial licensing requirements. |
| Submission Frequency | Applicants must submit a completed health questionnaire every two years. |
| Medical Consultation | If unsure about a question, applicants are advised to consult their physician. |
| Health Questions | The form contains 14 health-related questions that assess various medical conditions. |
| Physician Contact | Yes answers may require DMV to contact the applicant's physician regarding medical qualifications. |
| Certification Requirement | Applicants must certify that the information provided is true under penalty of perjury. |
| Governing Law | This form is governed by the California Vehicle Code, Section 12804.9. |
| Signature Requirement | Both the applicant and DMV examiner must sign and date the form for it to be valid. |
Filling out the California DMV DL 546 form is a straightforward process. This form requires you to answer several health-related questions to ensure you meet the necessary requirements for a driver's license. After completing the form, you will need to submit it to the DMV for review.
The California DMV DL 546 form is a health questionnaire designed to assess an applicant's medical qualifications for obtaining or renewing a driver's license. It helps ensure that individuals who may have medical conditions affecting their ability to drive safely are identified. This form is not applicable for commercial licensing requirements.
Applicants must submit a completed DL 546 form every two years. This requirement helps the DMV maintain updated health information to ensure that all drivers meet the necessary medical standards for safe driving.
If you answer "yes" to any of the health questions, you must provide an explanation in the space provided on the form or on a separate piece of paper. The DMV may need to contact your physician for further information regarding your medical qualifications before issuing a license.
If you are unsure how to answer a specific question on the DL 546 form, it is advisable to consult with your physician. They can provide guidance and help ensure that your responses accurately reflect your health status.
If you have a medical condition that may interfere with your ability to drive safely, it is crucial to disclose this on the DL 546 form. The DMV will review your health information and may require additional documentation or assessments to determine your eligibility for a driver's license.
Completing the California DMV DL 546 form can be a straightforward process, but there are common mistakes that applicants often make. One significant error is failing to provide complete and accurate personal information. It is crucial to ensure that your full name, address, date of birth, and driver license number are all correct. Any discrepancies can lead to delays or complications in processing your application.
Another frequent mistake is not answering the health questions thoroughly. Each question must be answered with a clear “yes” or “no.” Some applicants might skip questions or leave them blank, thinking they are not relevant. This can raise red flags during the review process. If you answer “yes” to any question, it is important to provide an explanation in the designated space or on an additional sheet of paper.
Many people also overlook the requirement to submit a completed health questionnaire every two years. Forgetting this can result in a lapse in your driving privileges. It is advisable to set reminders for yourself to ensure that you remain compliant with this requirement.
Additionally, applicants sometimes neglect to seek clarification from their physician when uncertain about how to answer a specific question. It is essential to consult your doctor if you are unsure. This not only helps you provide accurate information but also ensures that your medical qualifications are properly evaluated.
Some individuals may also fail to sign and date the form before submission. This is a critical step that confirms your acknowledgment of the information provided. Without a signature, the form may be considered incomplete, leading to further delays.
Lastly, not keeping a copy of the completed form for your records can be a mistake. Retaining a copy allows you to reference your answers in the future, especially if you are required to submit another health questionnaire or if there are questions about your application later on. Being proactive in this regard can save you time and stress down the line.
The California DMV DL 546 form, a health questionnaire, is essential for assessing an applicant's medical qualifications for a driver's license. Several other forms and documents often accompany this form, ensuring a comprehensive evaluation of an individual's ability to drive safely. Below is a list of related documents that may be needed.
These documents work together to ensure that all applicants meet the necessary health and safety standards before being issued a driver's license in California. It is important to have all relevant forms ready to facilitate a smooth application process.
When filling out the California DMV DL 546 form, it is essential to approach the process with care and attention to detail. Here are five things you should and shouldn't do:
The California DMV DL 546 form, known as the Health Questionnaire, is often surrounded by misunderstandings. Below are six common misconceptions regarding this form, along with clarifications to help individuals better understand its purpose and requirements.
This form must be completed by all applicants, regardless of their health status. It is designed to assess whether any health issues could affect driving ability.
Submission of the completed health questionnaire is mandatory every two years for those seeking to maintain their driver’s license in California.
The applicant is responsible for filling out the form. However, if uncertain about how to answer any questions, consulting a physician is advised.
While a "yes" answer may prompt further investigation, it does not guarantee disqualification. The DMV may contact the applicant's physician for clarification.
The DMV treats all medical information as confidential and only shares it with authorized personnel as necessary for evaluating the applicant’s fitness to drive.
All drivers, regardless of age, must complete the DL 546 form if they are renewing their license or if requested by the DMV.