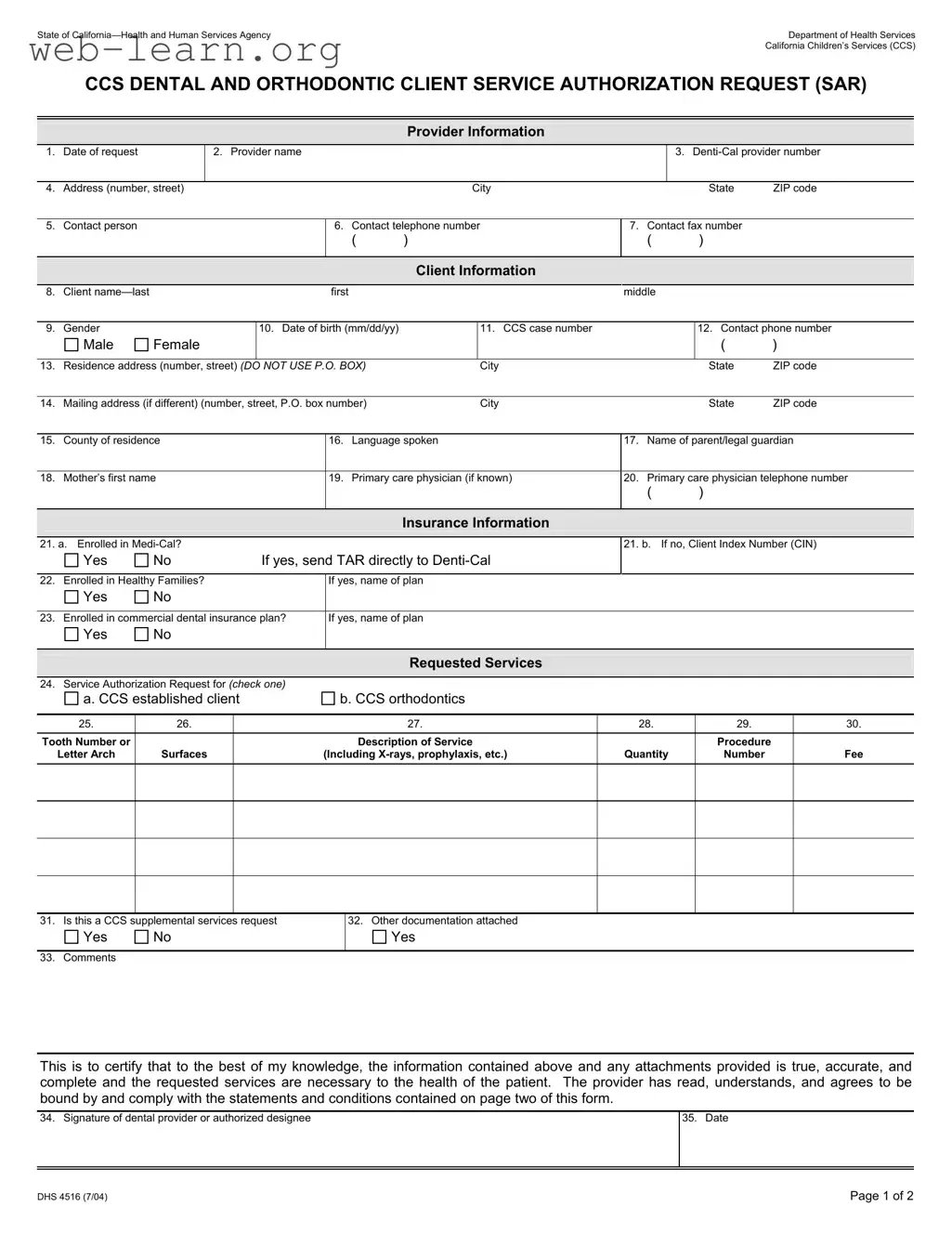
The California DHS 4516 form plays a crucial role in facilitating dental and orthodontic services for children enrolled in the California Children’s Services (CCS) program. This form is essential for providers seeking authorization for specific dental procedures, ensuring that necessary services are delivered to eligible clients. It includes sections for provider information, client details, insurance status, and a comprehensive list of requested services. Providers must fill out their contact information, the client's personal details, and any relevant insurance information, such as Medi-Cal or Healthy Families enrollment. Additionally, the form requires a detailed description of the requested services, including procedure codes, tooth numbers, and associated fees. The completion of this form not only verifies the necessity of the requested services but also certifies that the information provided is accurate and complete. By adhering to the guidelines outlined in the form, providers can help ensure that children receive the dental care they need in a timely manner.
| Fact Name | Description |
|---|---|
| Purpose | The DHS 4516 form is used to request service authorization for dental and orthodontic services for clients under California Children's Services (CCS). |
| Client Information | The form requires detailed client information, including name, date of birth, and residence address. This helps ensure that services are provided to the correct individual. |
| Insurance Details | Providers must indicate whether the client is enrolled in Medi-Cal or other insurance plans. This information is crucial for processing the request. |
| Governing Law | This form is governed by California Welfare and Institutions Code, Section 14000 et seq., which outlines the provisions for California Children's Services. |
| Signature Requirement | The form must be signed by the dental provider or an authorized designee, certifying that the information provided is accurate and complete. |
Completing the California DHS 4516 form requires careful attention to detail. Each section must be filled out accurately to ensure the request is processed smoothly. Follow the steps below to fill out the form correctly.
What is the purpose of the California DHS 4516 form?
The California DHS 4516 form, also known as the CCS Dental and Orthodontic Client Service Authorization Request (SAR), is used to request authorization for dental and orthodontic services for clients enrolled in California Children's Services (CCS). This form ensures that necessary services are approved before they are provided, which helps in managing costs and ensuring that clients receive appropriate care.
Who needs to fill out the DHS 4516 form?
The form must be completed by the dental provider or an authorized representative requesting services for a client. It requires detailed information about both the provider and the client, including personal details and insurance information. Accuracy is crucial, as the information provided will determine the approval of the requested services.
What information is required on the form?
The form requires several key pieces of information:
Each section must be filled out completely to avoid delays in processing.
What happens after the form is submitted?
Once the DHS 4516 form is submitted, it will be reviewed by the appropriate authority. If the requested services are approved, the provider will receive authorization to proceed with the treatment. If there are any issues or if additional information is needed, the provider may be contacted for clarification. It’s important to keep a copy of the submitted form for your records.
Filling out the California DHS 4516 form can be a straightforward process, but many people make common mistakes that can delay their requests. One frequent error is failing to provide the correct Denti-Cal provider number. This number is essential for processing the request, and any inaccuracies can lead to unnecessary delays.
Another common mistake is using a P.O. Box for the residence address. The form specifically instructs not to use P.O. Box numbers, yet many individuals overlook this requirement. Providing a physical address is crucial for accurate communication and service delivery.
Many people also forget to include the client’s date of birth in the correct format. The form requires the date to be entered as mm/dd/yy. Incorrect formatting can cause confusion and may result in the request being rejected.
In the insurance information section, some individuals mistakenly mark the wrong boxes regarding Medi-Cal enrollment. It’s important to carefully review the options. If the client is enrolled in Medi-Cal, the request should not be sent to CCS but directly to Denti-Cal.
Another frequent oversight is leaving out the CCS case number. If this number is unknown, it should be left blank rather than filled in incorrectly. An incorrect case number can lead to complications in processing the request.
When detailing the requested services, individuals often neglect to provide specific tooth numbers or descriptions. It’s vital to use the universal tooth code numbers or letters and include any necessary details about the services being requested. This information is key to ensuring that the right services are authorized.
Some applicants also fail to check the box indicating whether the request is for CCS supplemental services. This can lead to confusion about the nature of the request and may cause delays in approval.
Another mistake is not including a contact phone number for the client or legal guardian. This number is crucial for follow-up communications, and omitting it can hinder the process.
Lastly, individuals sometimes forget to sign the form or include the date of signature. The form must be signed by the dental provider or an authorized representative to be valid. Without a signature, the request cannot be processed.
By being aware of these common mistakes and taking the time to double-check the form, individuals can help ensure a smoother and more efficient submission process.
The California DHS 4516 form is a critical document used to request authorization for dental and orthodontic services for clients under the California Children's Services (CCS) program. Several other forms and documents often accompany this request, each serving a specific purpose in the authorization process. Below is a list of these documents.
Each of these documents plays a vital role in ensuring that the authorization process for dental and orthodontic services runs smoothly. Properly completing and submitting them can help facilitate timely access to necessary care for clients enrolled in the CCS program.
When filling out the California DHS 4516 form, there are important dos and don'ts to keep in mind. Here’s a helpful list:
Understanding the California DHS 4516 form can be challenging due to several misconceptions. Here are eight common misunderstandings explained:
By clarifying these misconceptions, individuals can better navigate the process of using the California DHS 4516 form and ensure that they are properly submitting requests for dental services.
Filling out the California DHS 4516 form can be a straightforward process if you keep a few key points in mind. This form is essential for requesting dental and orthodontic services for clients under the California Children’s Services (CCS) program. Here are some important takeaways to help you navigate the form effectively:
By keeping these points in mind, you can help streamline the process and ensure that your requests are processed efficiently. Filling out forms accurately not only saves time but also supports better care for clients.