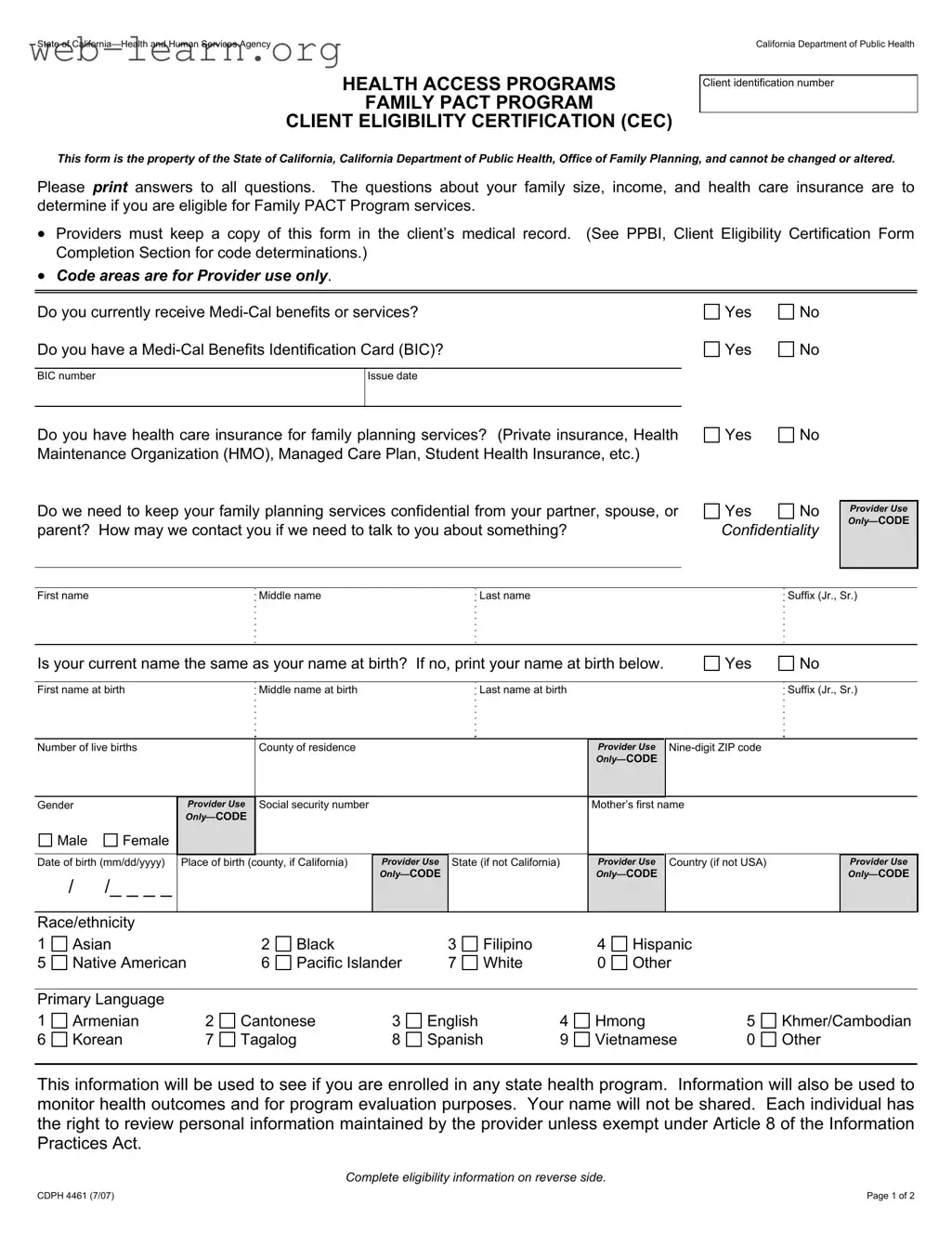
The California CDPH 4461 form, officially known as the Family PACT Program Client Eligibility Certification (CEC), plays a crucial role in ensuring access to family planning services for eligible individuals. Designed by the California Department of Public Health, this form gathers essential information about a client's family size, income, and health care insurance status. By answering questions regarding their current Medi-Cal benefits, private insurance, and confidentiality preferences, applicants can determine their eligibility for the Family PACT Program. Providers are required to maintain a copy of this form in the client's medical record, which aids in compliance and tracking. Additionally, the form includes sections for personal identification, income verification, and declarations regarding the accuracy of the information provided. The data collected not only assists in eligibility determinations but also contributes to health outcome monitoring and program evaluations, ensuring that the needs of the community are met effectively. Understanding the nuances of this form is vital for individuals seeking family planning assistance, as it lays the foundation for accessing necessary health services.
| Fact Name | Fact Description |
|---|---|
| Form Purpose | The CDPH 4461 form is used to determine eligibility for the Family PACT Program services. |
| Governing Law | This form is governed by California Health and Safety Code Section 24000. |
| Client Information | Clients must provide personal details, including family size, income, and health care insurance status. |
| Confidentiality | Clients can request confidentiality for their family planning services from partners or family members. |
| Provider Responsibilities | Providers are required to keep a copy of the completed form in the client's medical record. |
| Eligibility Review | Clients have the right to appeal decisions regarding their eligibility for services. |
| Signature Requirement | Applicants must sign the form, declaring the information provided is true and complete. |
Completing the California CDPH 4461 form is a crucial step in determining your eligibility for Family PACT Program services. Follow the steps carefully to ensure that all required information is accurately provided.
After completing the form, ensure that it is submitted to the appropriate provider. They will review your information and determine your eligibility for the Family PACT Program. Keep a copy for your records, as it may be needed for future reference.
The California CDPH 4461 form, also known as the Client Eligibility Certification (CEC), is used to determine eligibility for the Family PACT Program. This program provides family planning services to eligible individuals. The form collects essential information about the applicant's family size, income, and health care insurance status. By gathering this information, the program can assess whether the applicant qualifies for services.
Any individual seeking family planning services through the Family PACT Program must complete the CDPH 4461 form. This includes self, spouse, and children living in the household who are supported by the family income. It is important for applicants to provide accurate and complete information to ensure proper eligibility determination.
The form requires various details, including:
All answers must be printed clearly, and it is crucial to provide truthful information, as false statements may lead to ineligibility.
If your application for the Family PACT Program is denied, you have the right to appeal the decision. The process involves two steps:
It is important to follow the instructions carefully and meet all deadlines to ensure your appeal is considered.
Filling out the California CDPH 4461 form can be straightforward, but many make common mistakes that can lead to delays or ineligibility. One frequent error is failing to provide complete information. Each section of the form requires specific details about your family size, income, and health care insurance. Omitting any of these details can result in an incomplete application, leading to processing delays.
Another mistake is incorrect income reporting. Applicants often miscalculate their gross monthly income or fail to list all sources of income. This includes income from employment, self-employment, and other forms such as social security or child support. Ensure that all income sources are accounted for, as discrepancies can jeopardize eligibility.
Confusion about confidentiality is also a common issue. Some applicants do not clearly indicate whether they need their family planning services to remain confidential from partners or family members. This information is crucial for the provider to ensure your privacy. Be explicit in your response to avoid any misunderstandings.
Additionally, many individuals overlook the importance of signing the form. Without a signature, the application is not valid. This applies to both the applicant and any witnesses. Make sure that all necessary signatures are present before submitting the form to prevent delays in processing.
Lastly, failing to review the form before submission can lead to numerous errors. It is essential to double-check all entries for accuracy. Take the time to read through the completed form to ensure that all information is correct and complete. This simple step can save time and avoid potential issues with your application.
The California CDPH 4461 form is essential for determining eligibility for the Family PACT Program, which provides family planning services. However, several other documents may be required or useful in conjunction with this form. Understanding these documents can help ensure a smoother application process and better access to the services you need.
By being aware of these additional forms and documents, you can better navigate the application process for the Family PACT Program. Each document serves a specific purpose and contributes to a comprehensive understanding of your eligibility and rights. Always ensure that you have the necessary documentation ready to support your application and protect your interests.
The California CDPH 4461 form serves as a critical tool for determining eligibility for the Family PACT Program. Several other documents share similarities with this form in terms of purpose and required information. Here’s a list of five such documents:
When filling out the California CDPH 4461 form, there are several important practices to keep in mind. Here’s a list of what you should and shouldn’t do:
There are several misconceptions surrounding the California CDPH 4461 form. Understanding these can help applicants navigate the process more effectively. Below are nine common misconceptions:
By addressing these misconceptions, individuals can better understand the purpose of the CDPH 4461 form and the services available through the Family PACT Program.
Complete the form accurately. Use clear and legible handwriting to ensure that all information is easily understood.
Keep a copy of the form. Providers are required to maintain a copy in the client’s medical record for reference.
Confidentiality is important. Indicate if you need your family planning services to be kept confidential from your partner, spouse, or parent.
Be thorough when listing income. Include all sources of income, such as employment, social security, and any support payments.
Understand your rights. If you are denied eligibility, you have the right to appeal the decision through a first level review and a formal hearing.
Submit the form on time. Ensure that it is completed and submitted within the required timeframe to avoid delays in processing your application.