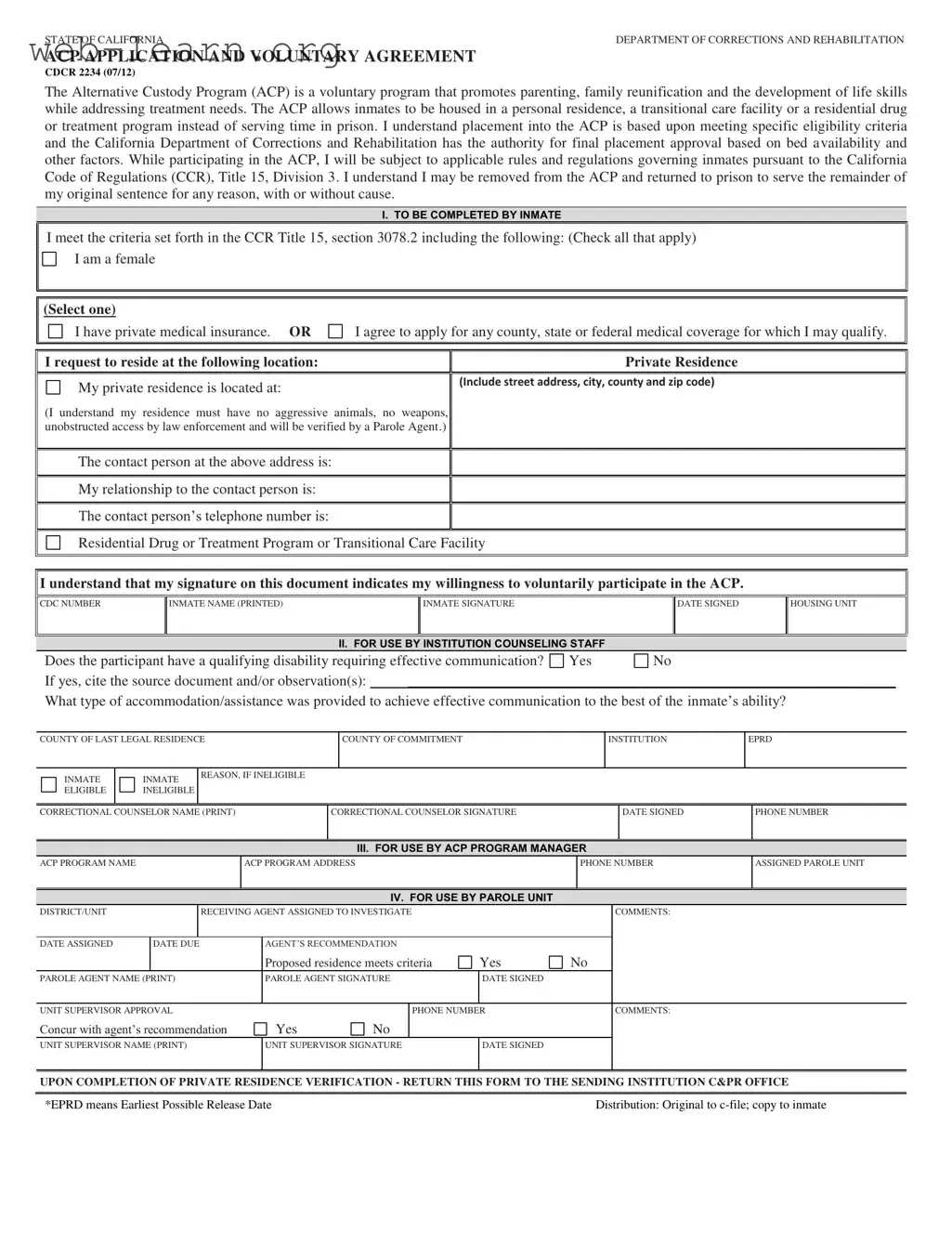
The California Alternative Custody Program (ACP) offers a transformative opportunity for eligible inmates seeking to reunite with their families while developing essential life skills. This voluntary program allows participants to serve their time in more supportive environments, such as their personal residences, transitional care facilities, or residential drug treatment programs, rather than within the confines of a traditional prison. The ACP is designed to address the treatment needs of inmates, fostering an atmosphere conducive to personal growth and family bonding. However, eligibility for this program is not universal; specific criteria must be met, and the final approval rests with the California Department of Corrections and Rehabilitation, which considers factors like bed availability. While enrolled in the ACP, participants must adhere to established rules and regulations, ensuring that the program maintains its integrity and effectiveness. Inmates must also understand that they can be returned to prison at any time for various reasons, emphasizing the importance of compliance and commitment to the program. The application process involves detailed information about the inmate's background, living arrangements, and any necessary accommodations, ensuring that the transition into alternative custody is as smooth as possible.
| Fact Name | Details |
|---|---|
| Program Purpose | The Alternative Custody Program (ACP) aims to support parenting, family reunification, and the development of life skills while addressing treatment needs for inmates. |
| Housing Options | Inmates can be housed in a personal residence, a transitional care facility, or a residential drug or treatment program instead of serving time in prison. |
| Eligibility Criteria | Eligibility for the ACP is determined by specific criteria outlined in the California Code of Regulations (CCR), Title 15, section 3078.2. |
| Authority and Removal | The California Department of Corrections and Rehabilitation has the final authority for placement approval. Inmates may be removed from the ACP and returned to prison for any reason, with or without cause. |
After completing the California Alternative Custody form, the next steps involve submitting the form to the appropriate authorities for review. This process ensures that all necessary information is evaluated, and eligibility is determined based on the criteria set forth by the California Department of Corrections and Rehabilitation.
The California Alternative Custody Program (ACP) is a voluntary initiative designed to support inmates in their roles as parents and to promote family reunification. It also focuses on helping inmates develop essential life skills while addressing their treatment needs. Instead of serving time in prison, eligible inmates can be housed in a personal residence, a transitional care facility, or a residential drug or treatment program.
To qualify for the ACP, inmates must meet specific criteria outlined in the California Code of Regulations (CCR), Title 15, section 3078.2. This includes being female, having private medical insurance, or agreeing to apply for available medical coverage. Additionally, the inmate must provide a suitable residence that meets safety and access requirements.
The chosen residence must adhere to certain conditions: it should not have aggressive animals, must be free of weapons, and should allow unobstructed access for law enforcement. The residence will be verified by a Parole Agent to ensure compliance with these requirements.
Yes, participation in the ACP is not guaranteed for the entire duration. Inmates can be removed from the program and returned to prison to serve the remainder of their original sentence for various reasons, which may include violations of program rules or other circumstances.
If an inmate has a qualifying disability that requires effective communication, the institution’s counseling staff must document this. They will also provide necessary accommodations to ensure the inmate can effectively participate in the program.
The Parole Agent plays a crucial role in the ACP. They are responsible for investigating the proposed residence, ensuring it meets all criteria, and making recommendations regarding the inmate's placement in the program. Their approval is essential for the inmate to participate.
Inmates interested in applying for the ACP must complete the required application form, indicating their willingness to participate voluntarily. They must also provide information about their proposed residence and any relevant medical coverage they may have or need to apply for.
Family members or friends can assist by ensuring the proposed residence meets the ACP requirements. They can also help the inmate gather necessary documentation, such as medical insurance information, and provide emotional support throughout the application process.
When filling out the California Alternative Custody form, many individuals make common mistakes that can delay or jeopardize their application. One frequent error is failing to check all applicable eligibility criteria. The form requires inmates to indicate if they meet specific conditions, such as being female or having private medical insurance. Missing even one box can lead to complications in the approval process.
Another mistake is providing incomplete or incorrect information regarding the proposed residence. The form asks for the full street address, city, county, and zip code. Omitting any of these details can result in rejection. Additionally, it's crucial to ensure that the residence meets the program’s safety requirements, such as having no aggressive animals or weapons.
Some applicants neglect to include a contact person at their proposed residence. This oversight can hinder the verification process. The form requires not just the contact person's name, but also their relationship to the inmate and a valid telephone number. Failing to provide this information can cause delays in the application review.
Inmates often forget to sign and date the form, which is a critical step. Without a signature, the application is considered incomplete. It's essential to double-check that the signature matches the printed name to avoid any confusion.
Another common error involves misunderstanding the eligibility requirements. Some inmates may assume they qualify without fully reviewing the criteria listed in the California Code of Regulations. This misunderstanding can lead to submitting an application that is ultimately deemed ineligible.
Additionally, applicants may overlook the section regarding disabilities and effective communication. If applicable, it’s vital to provide details about any accommodations that were made. Ignoring this section can result in unnecessary complications.
Some individuals fill out the form hastily, leading to typographical errors or unclear handwriting. Such mistakes can cause confusion and may require additional follow-up. Taking the time to write clearly and review the form can help prevent these issues.
Another mistake is not keeping a copy of the completed form. Without a record, it can be challenging to track the application status or provide additional information if needed. Keeping a copy is a simple but effective way to stay organized.
Lastly, failing to follow up after submitting the form can be detrimental. Applicants should be proactive in checking the status of their application to ensure it is being processed. Delays can occur, and staying informed can help address any issues quickly.
The California Alternative Custody Program (ACP) is a significant initiative designed to support inmates in their journey towards rehabilitation while allowing them to maintain family connections. Several forms and documents accompany the ACP application to ensure a comprehensive evaluation of eligibility and compliance with program requirements. Below is a list of related documents that are often utilized in conjunction with the California Alternative Custody form.
These documents collectively facilitate the assessment and approval process for inmates seeking to participate in the California Alternative Custody Program. They ensure that all necessary information is gathered to support the inmate's transition while prioritizing safety and compliance with program regulations.
The California Alternative Custody form shares similarities with several other legal documents designed for specific custody and rehabilitation purposes. Here are eight documents that are comparable:
When filling out the California Alternative Custody form, it is important to follow specific guidelines to ensure a smooth application process. Here are six things you should and shouldn't do:
Misconceptions about the California Alternative Custody form can lead to confusion and misinformed decisions. Here are nine common misunderstandings:
The ACP is entirely voluntary. Inmates can choose whether or not to participate based on their circumstances and eligibility.
Eligibility is determined by specific criteria outlined in the California Code of Regulations. Not every inmate will meet these requirements.
While the ACP may allow for a different living arrangement, it does not guarantee that an inmate will be released earlier than their original sentence.
The ACP is distinct from parole. It allows inmates to serve their time in a different environment, but they remain under the authority of the California Department of Corrections and Rehabilitation.
Inmates must propose a residence that meets specific criteria, including safety and accessibility for law enforcement verification.
Inmates can be removed from the ACP at any time for various reasons, including violations of rules or regulations.
Inmates in the ACP remain subject to rules and regulations governing inmates, and their activities are monitored by parole agents.
Inmates must either have private medical insurance or agree to apply for government medical coverage to qualify for the program.
While the form mentions female inmates, the ACP is available to eligible inmates of all genders, provided they meet the criteria.
Key Takeaways for Filling Out and Using the California Alternative Custody Form