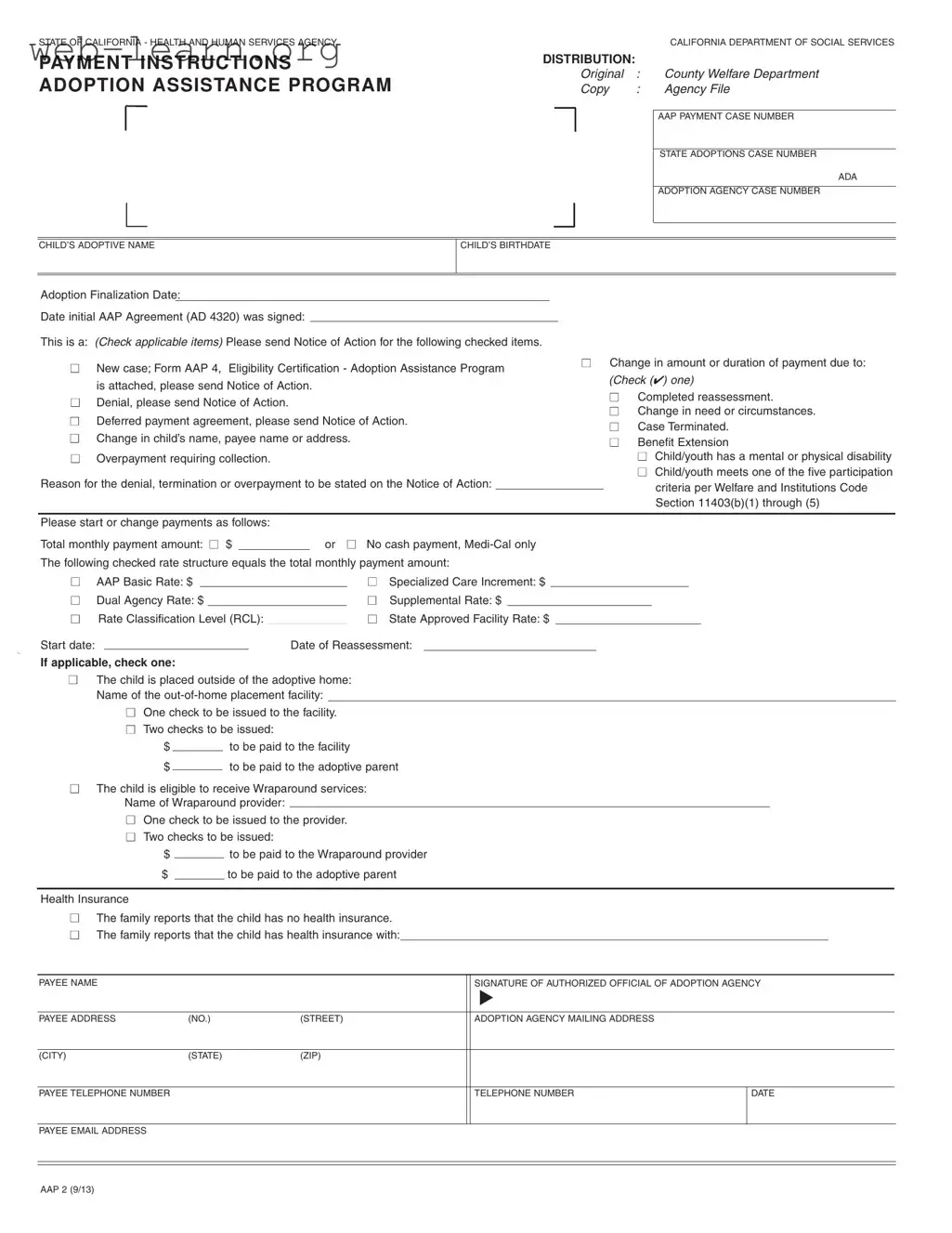
The California AAP 2 form plays a crucial role in the Adoption Assistance Program, designed to support families who have adopted children with special needs. This form is essential for initiating or modifying payment arrangements related to adoption assistance. It includes various sections where families can indicate important details such as the child's adoptive name, birthdate, and the date of adoption finalization. Families must also specify whether they are starting a new case or making changes to an existing agreement. The form allows for the submission of requests for payment adjustments, including changes in the payment amount or duration, and provides options for reporting circumstances like a child's disability or a change in family needs. Additionally, it outlines the necessary steps for processing payments, whether to the adoptive parent or to an out-of-home placement facility. Completing the AAP 2 form accurately and promptly is vital for ensuring that families receive the financial support they need during the adoption process.
| Fact Name | Details |
|---|---|
| Governing Law | The California AAP 2 form is governed by the Welfare and Institutions Code, specifically Section 11403, which outlines the Adoption Assistance Program. |
| Purpose | This form is used to request or change payments under the Adoption Assistance Program for children placed in adoptive homes. |
| Distribution | Upon completion, the original form is submitted to the County Welfare Department, while a copy is retained in the agency file. |
| Eligibility Criteria | Eligibility for assistance includes children with mental or physical disabilities and those meeting specific participation criteria outlined in the governing law. |
| Payment Structure | The form allows for various payment structures, including the AAP Basic Rate, Specialized Care Increment, and others, which must be detailed in the payment section. |
| Health Insurance Disclosure | Families must indicate whether the child has health insurance, which is essential for determining the overall support package. |
Completing the California AAP 2 form requires attention to detail and accuracy. Once filled out, this form will be submitted to the appropriate county welfare department to initiate or modify the adoption assistance payments. Follow the steps below to ensure the form is completed correctly.
What is the purpose of the California AAP 2 form?
The California AAP 2 form is used in the Adoption Assistance Program. It helps families apply for or change their adoption assistance payments. This form collects important information about the child, the adoptive family, and any changes in circumstances that might affect the payment amount or eligibility.
Who needs to fill out the AAP 2 form?
The form must be completed by the adoptive parent or guardian of the child. Additionally, an authorized official from the adoption agency must also sign the form. This ensures that all information is verified and correct before submitting it to the county welfare department.
What information is required on the AAP 2 form?
Several key details are needed on the AAP 2 form:
This information helps the county welfare department process the request efficiently.
What should I do if my circumstances change after submitting the AAP 2 form?
If your circumstances change, you should fill out a new AAP 2 form to reflect those changes. This includes changes in the child's name, payment amount, or any other relevant details. It is crucial to keep the county welfare department informed to ensure that assistance payments remain accurate and timely.
Completing the California AAP 2 form can be a straightforward process, yet many individuals encounter common pitfalls. One significant mistake is failing to provide accurate information regarding the child's adoptive name and birthdate. These details are crucial for the processing of the adoption assistance application. Inaccuracies can lead to delays or even denials of benefits, as the information must align with official records. It is essential to double-check these entries to ensure they are correct and complete.
Another frequent error occurs when individuals neglect to indicate the specific reason for changes in payment or circumstances. The form requires a clear explanation of any modifications, such as changes in the child’s needs or circumstances. Without this information, the county welfare department may struggle to process the request efficiently. Providing a detailed rationale not only aids in the approval process but also helps in establishing a clear record of the child's situation.
Moreover, many applicants overlook the importance of including the correct payment structure. The form provides various options for payment amounts and structures, such as the AAP Basic Rate or Specialized Care Increment. Failing to check the appropriate boxes or miscalculating the total monthly payment can result in incorrect payments or delays in processing. It is advisable to carefully review the payment section to ensure all amounts are accurately represented and reflect the family's needs.
Lastly, individuals often forget to sign the form or include the necessary contact information. A signature is not just a formality; it serves as a confirmation that the information provided is accurate and complete. Additionally, including a current phone number and email address allows the agency to reach out for any clarifications or additional information needed. Omitting these details can lead to unnecessary complications and hinder the timely processing of the application.
The California AAP 2 form is a crucial document in the Adoption Assistance Program, facilitating financial support for adoptive families. When navigating this process, several other forms and documents may be needed to ensure everything runs smoothly. Here are four key documents that are often used alongside the AAP 2 form.
Being aware of these additional documents can significantly ease the process of applying for and managing adoption assistance in California. Each form plays a vital role in ensuring that families receive the support they need during this important transition.
The California AAP 2 form is an important document used in the Adoption Assistance Program. It serves various functions, similar to several other forms used in adoption and assistance processes. Below are eight documents that share similarities with the AAP 2 form, along with explanations of how they relate to it.
Understanding these documents and their similarities can help families navigate the adoption assistance process more effectively. Each form plays a crucial role in ensuring that children and their adoptive families receive the support they need.
When filling out the California AAP 2 form, it’s important to be thorough and accurate. Here are some essential dos and don’ts to keep in mind:
Following these guidelines can help ensure a smoother process when applying for adoption assistance in California.
Understanding the California AAP 2 form can be challenging, and misconceptions can lead to confusion. Here are seven common misunderstandings about this important document:
By understanding these misconceptions, families can navigate the adoption assistance process more effectively and ensure they receive the benefits they deserve.
Filling out the California AAP 2 form is a crucial step in accessing adoption assistance. Here are key takeaways to consider:
Completing the AAP 2 form accurately and thoroughly can facilitate a smoother process in receiving adoption assistance benefits.