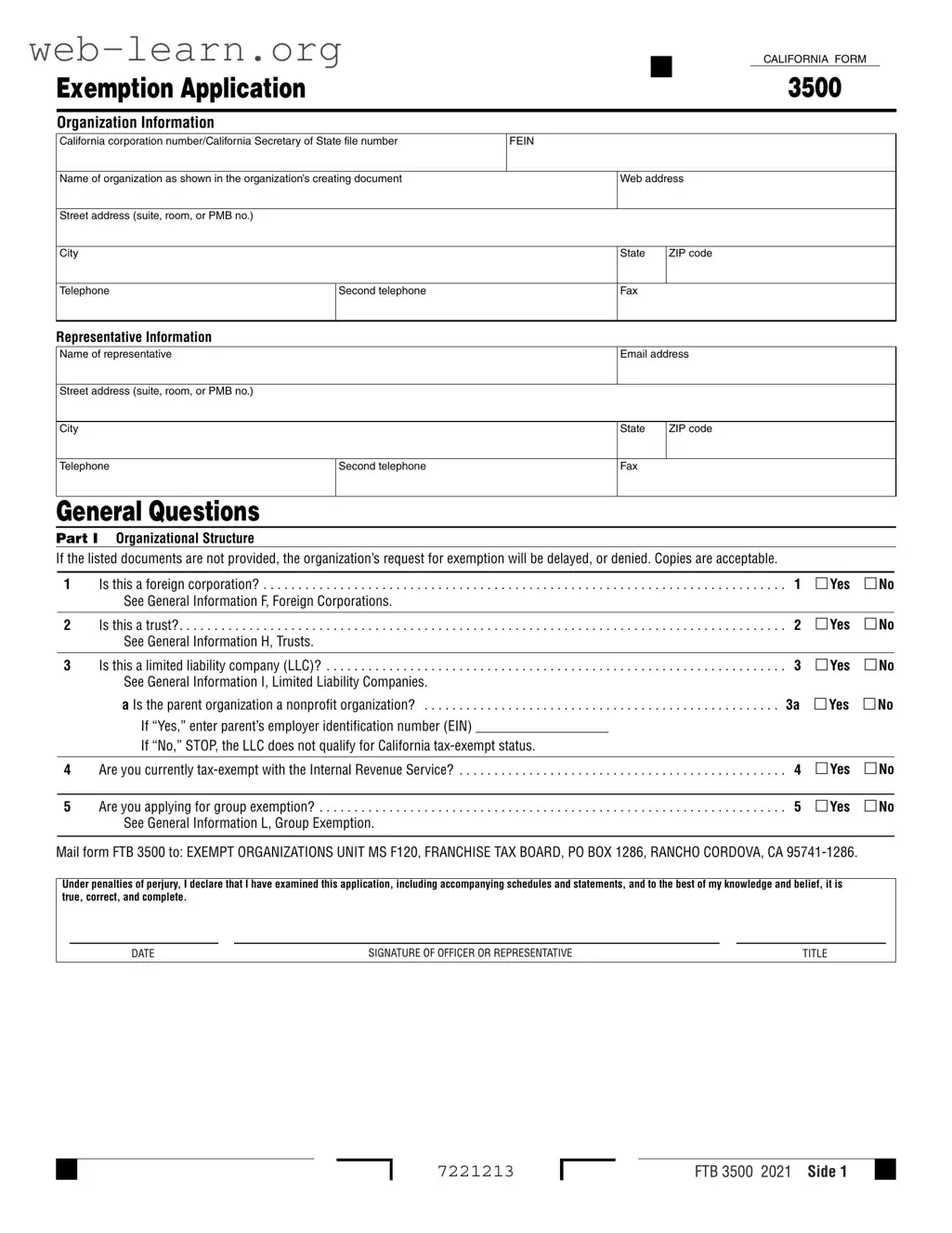
The California 3500 form is a crucial document for organizations seeking tax-exempt status in the state of California. This form, officially known as the Exemption Application, collects essential information about the organization, including its structure, activities, and financial data. To begin, organizations must provide their basic details, such as the California corporation number, federal employer identification number (FEIN), and contact information. Additionally, the form includes a series of questions that help determine the organization's eligibility for exemption. These questions cover various aspects, such as whether the organization is a foreign corporation, trust, or limited liability company (LLC), and whether it is currently recognized as tax-exempt by the Internal Revenue Service (IRS). The form also requires a narrative description of the organization's activities, outlining past, present, and future plans, which is vital for demonstrating how the organization fulfills its exempt purpose. Furthermore, financial data, including annual returns and compensation for officers, is necessary for the review process. Lastly, the form emphasizes the importance of providing complete and accurate information, as any missing documentation may delay or deny the exemption request. Understanding these components is essential for organizations aiming to navigate the complexities of California's tax-exempt application process successfully.



| Fact Name | Description |
|---|---|
| Purpose of Form | The California Form 3500 is an Exemption Application used by organizations to apply for tax-exempt status in California. |
| Governing Law | This form is governed by the California Revenue and Taxation Code, specifically sections related to tax-exempt organizations. |
| Eligibility Criteria | Organizations must meet specific criteria, such as being a nonprofit, to qualify for tax exemption. |
| Required Information | Applicants must provide detailed information about their organizational structure, activities, and financial data. |
| Submission Address | Completed forms should be mailed to the Exempt Organizations Unit at the Franchise Tax Board in Rancho Cordova, CA. |
| Review Process | The Franchise Tax Board reviews the submitted information to determine eligibility for tax-exempt status. |
| Potential Delays | Failure to provide necessary documents may result in delays or denial of the exemption request. |
Filling out the California 3500 form requires careful attention to detail. It is essential to provide accurate information about your organization and its activities. Make sure you have all necessary documents ready, as missing information can delay your application.
Once completed, mail the form to the Exempt Organizations Unit at the address provided. Make sure to keep a copy for your records. This submission is a crucial step in seeking tax-exempt status for your organization.
What is the California 3500 form?
The California 3500 form is an exemption application used by organizations seeking tax-exempt status in California. This form is submitted to the Franchise Tax Board and requires detailed information about the organization, its structure, activities, and financial data.
Who needs to file the California 3500 form?
Any organization that wishes to obtain or maintain tax-exempt status in California must file the California 3500 form. This includes corporations, trusts, and limited liability companies (LLCs) that meet specific criteria for exemption.
What information is required on the California 3500 form?
The form requires a variety of information, including:
How does an organization demonstrate its tax-exempt purpose?
Organizations must provide a detailed narrative of their activities that shows how they further their exempt purpose. This includes a description of each activity, its purpose, and the resources allocated to it. The form also requires the organization to indicate the percentage of time spent on each activity.
What happens if the California 3500 form is incomplete?
If the form is incomplete or if required documents are not provided, the organization’s request for exemption may be delayed or denied. It is essential to ensure that all sections are filled out accurately and that any necessary attachments are included.
Can an organization apply for group exemption using the California 3500 form?
Yes, organizations can apply for group exemption on the California 3500 form. If an organization is part of a larger group, it must indicate this on the form and provide any additional documentation required to support the group exemption request.
What is the significance of the organization’s financial data?
The financial data provided on the California 3500 form is crucial for determining the organization’s eligibility for tax-exempt status. Organizations must report their income and expenses for the current year and the previous three years. If the organization has not yet started operations, a proposed budget for the next four years is required.
What should be done if the organization’s tax-exempt status was previously revoked?
If the organization’s tax-exempt status was previously revoked, it must provide the date of revocation on the form. The organization may need to provide additional information or documentation to demonstrate its current eligibility for tax-exempt status.
Where should the completed California 3500 form be sent?
The completed California 3500 form should be mailed to the Exempt Organizations Unit at the Franchise Tax Board. The address is:
Exempt Organizations Unit
MS F120, Franchise Tax Board
PO Box 1286
Rancho Cordova, CA 95741-1286
Filling out the California Form 3500 can be a straightforward process, but there are common mistakes that applicants often make. Recognizing these pitfalls can help ensure that your application is processed smoothly and efficiently.
One frequent error is neglecting to provide necessary documentation. The form clearly states that certain documents must accompany the application. If these documents are missing, it can lead to delays or even denial of the exemption request. Always double-check that you have included all required copies, as incomplete submissions will hinder your application.
Another mistake involves misidentifying the organization’s structure. Applicants sometimes fail to accurately answer questions regarding whether they are a foreign corporation, a trust, or a limited liability company (LLC). Misclassification can lead to confusion and may affect the eligibility for tax-exempt status. It is vital to understand the nature of your organization before completing this section.
Inaccurate or incomplete answers to the general questions can also be problematic. For instance, stating that your organization is not currently tax-exempt with the IRS when it actually is can result in significant complications. Each question must be answered truthfully and completely to avoid future issues.
Furthermore, failing to provide a detailed narrative of activities is a common oversight. The form requires a comprehensive description of past, present, and planned activities. Simply repeating language from the organizational document is insufficient. Each activity should be explained in detail, including its purpose and how it aligns with the organization's exempt purpose.
Another area where applicants often falter is in the financial data section. It is crucial to ensure that all required financial information is accurate and complete. Missing or incorrect figures can raise red flags and delay the review process. Providing a detailed income and expense statement, as well as any proposed budgets, is essential for demonstrating financial accountability.
Lastly, applicants frequently overlook the importance of listing all officers, directors, and trustees accurately. This section requires the names, titles, and compensation details of all individuals involved with the organization. Omitting this information or providing inaccurate details can lead to complications in the approval process. Make sure to double-check this section for accuracy before submission.
By being mindful of these common mistakes, applicants can improve their chances of a successful and timely application process. Attention to detail and thoroughness are key to navigating the California Form 3500 effectively.
The California Form 3500 is an essential document for organizations seeking tax-exempt status in California. When completing this form, you may also need to prepare additional documents to support your application. Here are five common forms and documents often used alongside the California 3500 form, each serving a specific purpose in the exemption application process.
Each of these documents plays a significant role in the exemption application process. Ensuring that you have all necessary forms and supporting materials ready can help streamline your application and increase the likelihood of a favorable outcome. It is important to review each requirement carefully and provide accurate information to avoid delays or potential denials in your application for tax-exempt status.
The California Form 3500 is an important document used by organizations seeking tax-exempt status. Several other forms share similarities with the California 3500 in terms of purpose and structure. Here’s a list of nine documents that are comparable:
Each of these forms plays a crucial role in the process of maintaining or obtaining tax-exempt status, and they require organizations to provide detailed information about their structure, activities, and finances.
When filling out the California Form 3500, it is essential to follow specific guidelines to ensure a smooth application process. Below is a list of things you should and should not do.
While the California 3500 form is primarily used by nonprofit organizations seeking tax-exempt status, it can also apply to certain other entities, such as trusts and limited liability companies (LLCs), under specific conditions. Therefore, it’s crucial to review the eligibility criteria before assuming that only nonprofits can use this form.
This is not true. The form requires various supporting documents to be included with the application. If these documents are missing, the request for exemption may be delayed or even denied. It's essential to gather all necessary documentation beforehand to ensure a smooth application process.
Submitting the form does not guarantee tax-exempt status. The Franchise Tax Board reviews the application and supporting materials thoroughly. If any discrepancies or issues arise, the application may be denied, or additional information may be requested. Therefore, it’s important to provide accurate and complete information from the start.
This is a common misunderstanding. Even if an organization has been denied tax-exempt status in the past, it can still reapply. However, it must address the reasons for the previous denial and demonstrate how it has rectified those issues. Persistence and careful attention to the application process can lead to a successful outcome.
When filling out the California Form 3500, there are several important aspects to keep in mind to ensure a smooth application process. Here are key takeaways to consider:
By following these guidelines, you can help ensure that your Form 3500 is completed correctly and submitted successfully.