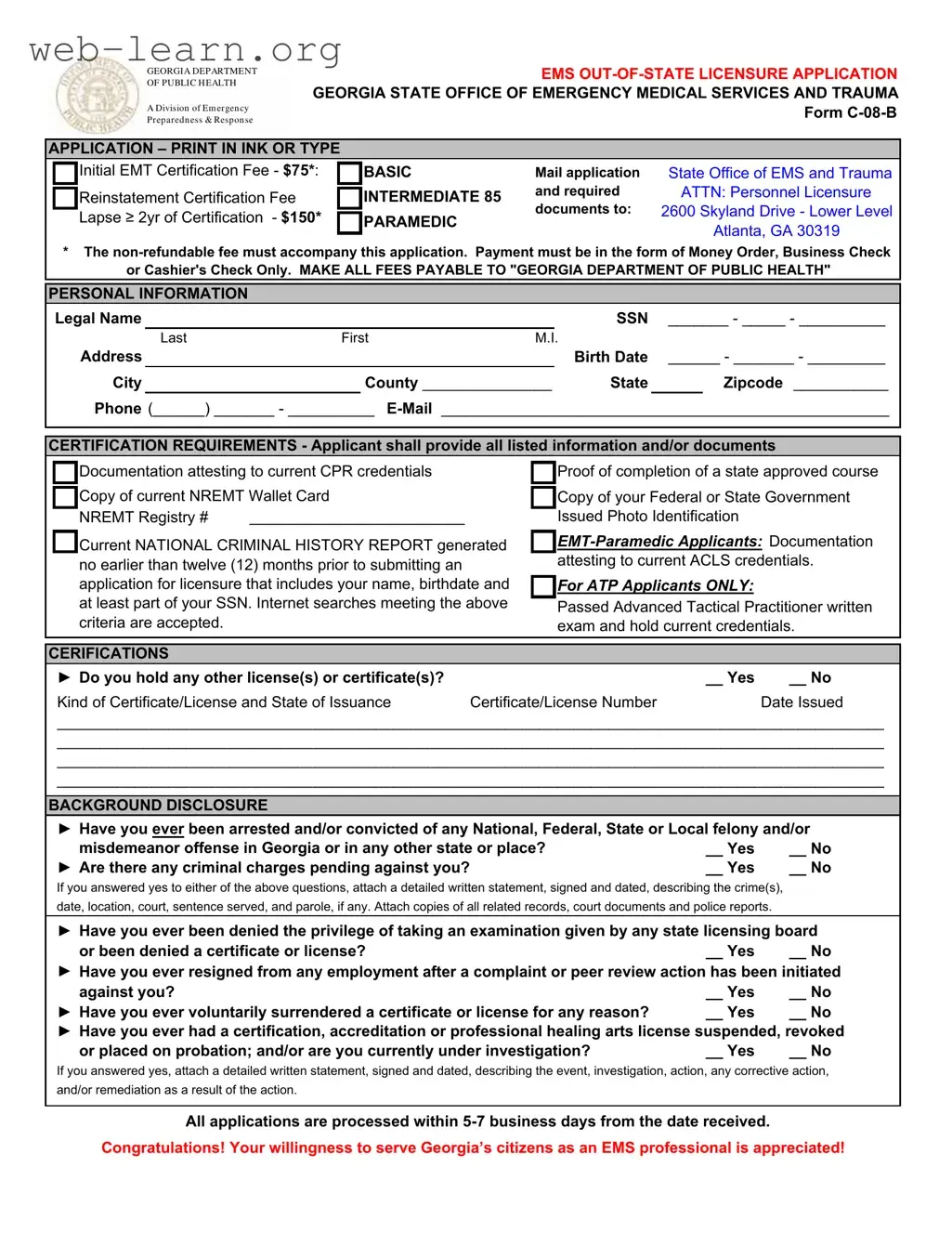
The C 08 B Georgia form is a crucial document for individuals seeking out-of-state licensure as Emergency Medical Services (EMS) professionals in Georgia. This application serves multiple purposes, primarily facilitating the certification process for EMTs, paramedics, and other EMS providers who are licensed in other states. Applicants must submit a completed form along with a non-refundable fee, which varies depending on their level of certification—$75 for Basic, $85 for Intermediate, and $150 for those whose certification has lapsed for two years or more. Essential personal information, including legal name, Social Security number, and contact details, must be clearly provided. Additionally, the form requires documentation that attests to the applicant's current CPR credentials, completion of a state-approved course, and a valid National Registry of Emergency Medical Technicians (NREMT) card. Background disclosures are also a critical component, where applicants must disclose any past criminal offenses or licensing issues. The application process is designed to ensure that only qualified individuals are granted the privilege to serve Georgia's citizens in emergency medical situations, reflecting the state's commitment to public health and safety.

| Fact Name | Details |
|---|---|
| Form Title | EMS Out-of-State Licensure Application |
| Governing Body | Georgia Department of Public Health |
| Application Fees | Initial EMT Certification Fee: $75; Intermediate: $85; Paramedic: $150 (non-refundable) |
| Submission Address | 2600 Skyland Drive - Lower Level, Atlanta, GA 30319 |
| Processing Time | Applications are processed within 5-7 business days from receipt. |
| Required Documents | Current CPR credentials, NREMT Wallet Card, Federal or State ID, and National Criminal History Report. |
| Background Disclosure | Applicants must disclose any arrests or convictions and provide details if applicable. |
| Notary Requirement | Application must be notarized only if a passport photograph is attached. |
To complete the C 08 B Georgia form for out-of-state licensure, follow these steps carefully. Ensure that all required information is accurate and complete. Once the form is filled out, it will be submitted to the Georgia Department of Public Health along with the necessary fees and documents.
After submission, the application will be processed within 5-7 business days. It is important to ensure that all information is accurate to avoid delays in the licensure process.
What is the purpose of the C 08 B Georgia form?
The C 08 B form is an application for out-of-state licensure for Emergency Medical Technicians (EMTs) in Georgia. It is specifically designed for individuals who are seeking to obtain licensure to practice as EMTs in Georgia while holding a certification or license from another state.
What fees are associated with submitting the C 08 B form?
Applicants must pay a non-refundable fee when submitting the form. The fees are as follows:
Payments must be made via money order, business check, or cashier's check, and should be made payable to the "Georgia Department of Public Health."
What personal information is required on the application?
Applicants must provide their legal name, Social Security Number (SSN), address, birth date, phone number, and email address. This information is essential for processing the application and verifying the applicant's identity.
What documents must be submitted with the application?
Along with the completed application form, applicants need to submit several documents, including:
For EMT-Paramedic applicants, documentation attesting to current Advanced Cardiac Life Support (ACLS) credentials is also required.
What should I do if I have a criminal record?
If you have ever been arrested or convicted of a felony or misdemeanor, you must answer "yes" to the relevant questions on the application. You will need to attach a detailed written statement describing the crime, including the date, location, court, and any sentences served. Copies of related records and documents should also be included.
How long does it take to process the application?
All applications are processed within 5 to 7 business days from the date they are received. It is important to ensure that all required documents and fees are submitted to avoid delays in processing.
What happens after my application is approved?
Once the application is approved, the applicant will receive a license to practice as an EMT in Georgia. This licensure allows the individual to serve the community as an EMS professional, contributing to public health and safety.
Is there an affidavit that needs to be signed?
Yes, the application includes an affidavit where the applicant acknowledges that they have read and answered all questions truthfully. The applicant also consents to an investigation of their moral character and professional reputation as part of the licensing process.
Completing the C 08 B Georgia form is a crucial step for those seeking out-of-state licensure as an EMS provider. However, many applicants make common mistakes that can delay the processing of their application. Understanding these pitfalls can save time and ensure a smoother application experience.
One frequent error involves the payment method. The application requires fees to be paid via money order, business check, or cashier's check. Many applicants mistakenly send personal checks or cash, which can lead to immediate rejection of the application. It is essential to follow the specified payment instructions closely to avoid such issues.
Another common mistake is providing incomplete personal information. Applicants often forget to fill in critical details, such as their Social Security Number or contact information. Missing information can halt the processing of the application, so double-checking all fields before submission is advisable.
Some individuals neglect to include the necessary documentation that supports their application. This includes proof of CPR certification, NREMT wallet card, and a national criminal history report. Failing to attach these documents can result in delays or outright denial of the application. Ensuring that all required documents are included is vital for a successful submission.
In addition, applicants sometimes overlook the importance of background disclosure. Failing to disclose past criminal history or disciplinary actions can lead to serious consequences, including potential legal ramifications. It is better to be transparent and provide a detailed statement if any such issues exist.
Moreover, some applicants forget to sign and date the affidavit section of the application. This step is crucial, as it confirms the accuracy of the information provided. An unsigned application may be considered incomplete, leading to further delays.
Another mistake is the failure to follow instructions regarding notarization. The application clearly states that the notary should not sign unless a passport photograph is attached. Ignoring this requirement can complicate the process, as the application may be returned for correction.
Some applicants also misinterpret the section about holding other licenses. They may either fail to disclose additional licenses or provide insufficient details about them. Complete and accurate reporting of all certifications is essential to avoid complications in the review process.
Finally, many people underestimate the importance of timeliness in submitting their application. The process can take 5-7 business days, but delays can occur if the application is incomplete or incorrect. Submitting the application well in advance of any deadlines is a wise strategy.
By being aware of these common mistakes, applicants can navigate the C 08 B Georgia form with greater ease and confidence. Attention to detail and adherence to instructions are key components of a successful application process.
The C 08 B form is essential for individuals seeking licensure as Emergency Medical Technicians (EMTs) in Georgia. Alongside this form, several other documents are typically required to ensure a complete application. Below is a list of these documents, each playing a crucial role in the licensure process.
These documents collectively support the C 08 B form, helping to establish the qualifications and background of applicants. Properly completing and submitting these forms is crucial for a smooth licensure process in Georgia.
The C 08 B Georgia form is an application for out-of-state licensure for Emergency Medical Services (EMS) professionals. Several other documents serve similar purposes in various contexts. Here are six documents that share similarities with the C 08 B form:
Each of these documents plays a crucial role in ensuring that EMS professionals meet the necessary standards for practice and maintain the safety and well-being of the communities they serve.
When filling out the C 08 B Georgia form, there are important guidelines to follow. Here’s a list of things you should and shouldn't do:
Following these guidelines will help ensure your application is processed smoothly.
This form is actually designed for both initial certification and reinstatement of licensure. If someone has previously held a license that has lapsed, they can use this form to apply for reinstatement as well.
In reality, the application fee must be paid using specific methods. Acceptable forms include a money order, business check, or cashier's check only. Personal checks are not accepted, which is a common misunderstanding.
Many people believe that answering background questions is optional. However, providing accurate information about any arrests or convictions is mandatory. Failure to disclose this information can lead to denial of the application.
Applicants often think that their applications will be processed right away. In fact, the processing time typically ranges from 5 to 7 business days from the date the application is received.
This form is not limited to EMTs. It is applicable to various levels of emergency medical service providers, including paramedics and advanced tactical practitioners. Each category has specific requirements that must be met.
Filling out and using the C 08 B Georgia form for out-of-state licensure as an EMS provider requires careful attention to detail. Here are some key takeaways to guide you through the process:
By following these key takeaways, you can navigate the C 08 B Georgia form process more effectively, ensuring that your application for EMS licensure is complete and compliant with state requirements.