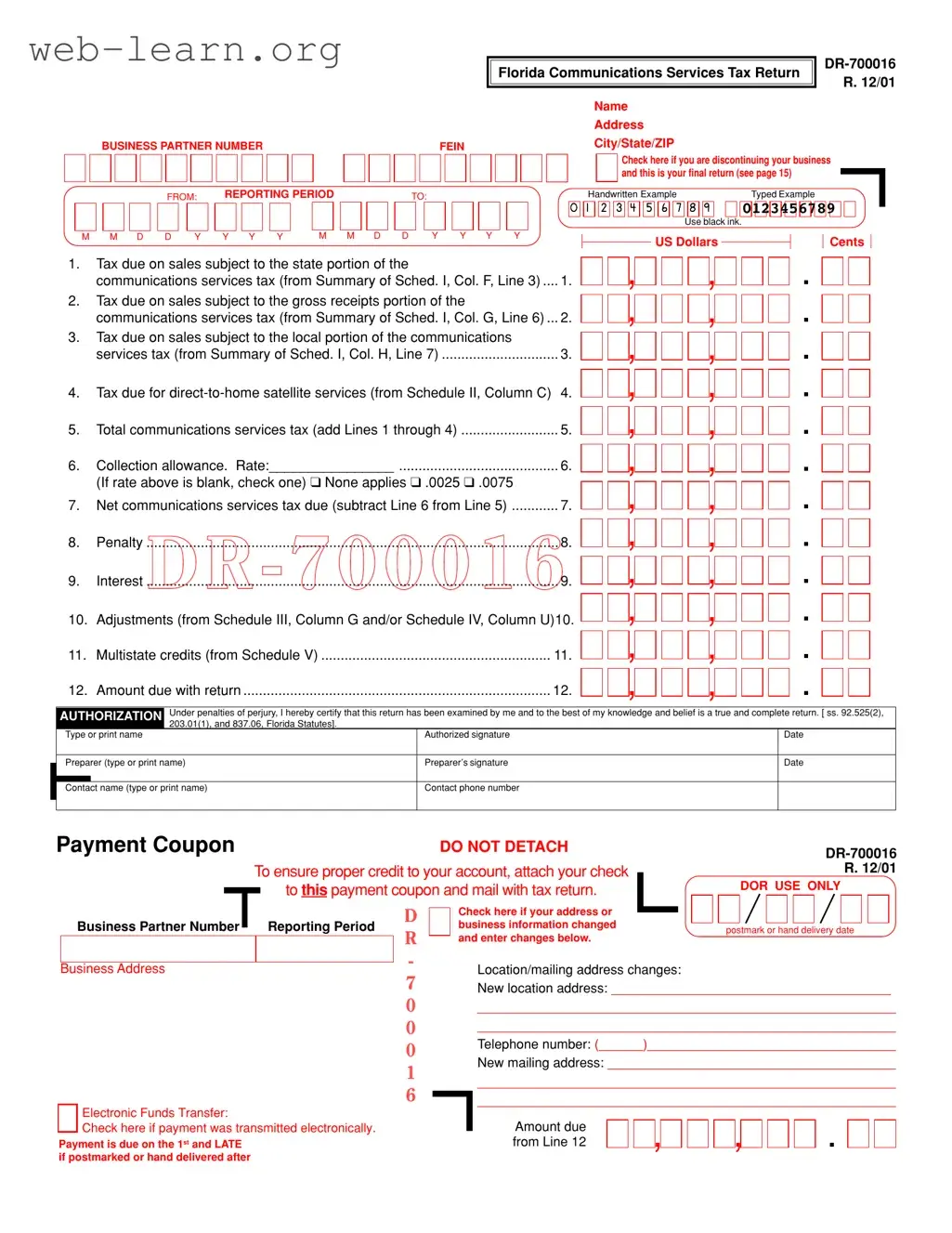
The Business Partner Number Florida form, officially designated as DR-700016, is an essential document for businesses operating within the state that are subject to the communications services tax. This form collects vital information such as the business name, address, and the unique Business Partner Number, which identifies the entity for tax purposes. It is crucial for businesses to accurately report their tax liabilities, including amounts due on sales subject to various tax categories, such as state, gross receipts, and local taxes. The form also includes sections for adjustments, penalties, and interest, ensuring comprehensive reporting. Additionally, businesses must indicate whether this submission is their final return if they are discontinuing operations. The form facilitates electronic filing, which the Florida Department of Revenue encourages for its efficiency and accuracy. Timely submission is imperative, as payments are due on the first of each month and may incur penalties if postmarked late. Completing this form correctly ensures compliance with state tax laws and contributes to the overall financial health of the business.

| Fact Name | Details |
|---|---|
| Form Name | Florida Communications Services Tax Return (Form DR-700016) |
| Purpose | This form is used to report and pay the communications services tax in Florida. |
| Business Partner Number | A unique identifier assigned to each business for tax purposes. |
| Filing Frequency | Businesses must file this return periodically, depending on their reporting period. |
| Governing Laws | Florida Statutes Sections 92.525(2), 203.01(1), and 837.06 govern this form. |
| Payment Methods | Payments can be made via check, electronic funds transfer, or online filing. |
| Final Return Option | There is a checkbox for indicating if this is the final return due to business discontinuation. |
| Contact Information | Contact details must be provided for assistance and inquiries regarding the form. |
Filling out the Business Partner Number Florida form is an important step for businesses operating in the state. This form requires specific information about your business and tax obligations. To ensure accuracy and compliance, follow these steps carefully.
After submitting your form, keep a copy for your records. If you have any questions or need assistance, consider reaching out to the Florida Department of Revenue or consult a tax professional.
What is the Business Partner Number Florida form?
The Business Partner Number Florida form, also known as DR-700016, is used by businesses to report and pay the communications services tax in Florida. This form collects information about taxable sales and the taxes owed to the state and local jurisdictions.
Who needs to file this form?
Any business that provides communications services in Florida must file this form. If your business collects communications services tax from customers, you are required to report and remit these taxes to the Florida Department of Revenue.
What information is required on the form?
The form requires several pieces of information, including:
Make sure to provide accurate figures to avoid penalties.
How do I calculate the taxes due?
To calculate the taxes due, you need to add up the taxes from various categories, including:
After totaling these amounts, you can apply any collection allowance and determine the net tax due.
What if I am discontinuing my business?
If you are discontinuing your business, check the box on the form indicating that this is your final return. This informs the Florida Department of Revenue that you are no longer operating and ensures that your account is properly closed.
How do I submit the form?
You can submit the Business Partner Number Florida form either by mail or electronically. To file by mail, send the completed form along with any payment to:
Florida Department of Revenue
PO Box 6520
Tallahassee, FL 32314-6520
For electronic filing, visit www.myflorida.com/dor to file online.
What are the penalties for late filing?
If you file the form after the due date, you may incur penalties and interest on the amount due. It is important to file on time to avoid these additional charges.
Who can I contact for assistance?
If you have questions or need assistance, you can contact the Florida Department of Revenue’s e-Services Unit at 1-800-352-3671 (within Florida) or 850-487-7972. They can provide guidance on filing and payment processes.
When filling out the Business Partner Number Florida form, individuals often make several common mistakes that can lead to processing delays or incorrect submissions. One frequent error is not using black ink when completing the form. The instructions specify that black ink should be used, and failing to follow this guideline can result in the form being unreadable by processing equipment.
Another mistake involves inaccurate or incomplete information regarding the business partner number. This number is crucial for identifying the business entity. If the number is incorrect or missing, it can cause significant issues with tax processing and compliance. Ensuring that this information is entered correctly is essential.
Additionally, individuals sometimes neglect to check the appropriate box if they are discontinuing their business. This step is important, as it indicates that the return being filed is the final one. Not marking this can lead to confusion about the business's status and potential future tax obligations.
Lastly, many people overlook the requirement to provide a signature and date on the form. An unsigned form is considered incomplete and may be rejected. It is important to remember that both the preparer and the authorized person must sign and date the return to validate it.
The Business Partner Number Florida form is essential for businesses operating within the state, particularly for those involved in providing communication services. However, several other forms and documents are often necessary to ensure compliance with state regulations. Below is a list of these related documents, each serving a specific purpose in the business registration and tax reporting process.
Understanding these forms and their purposes can significantly aid businesses in maintaining compliance with Florida's tax regulations. Each document plays a crucial role in ensuring that businesses operate smoothly and fulfill their tax obligations effectively.
The Business Partner Number Florida form shares similarities with several other documents that are essential for business operations and tax compliance. Below is a list of eight documents that have comparable functions or requirements.
When filling out the Business Partner Number Florida form, there are several important practices to follow. Here’s a list of things you should and shouldn't do:
Here are six common misconceptions about the Business Partner Number Florida form:
Here are some key takeaways for filling out and using the Business Partner Number Florida form: