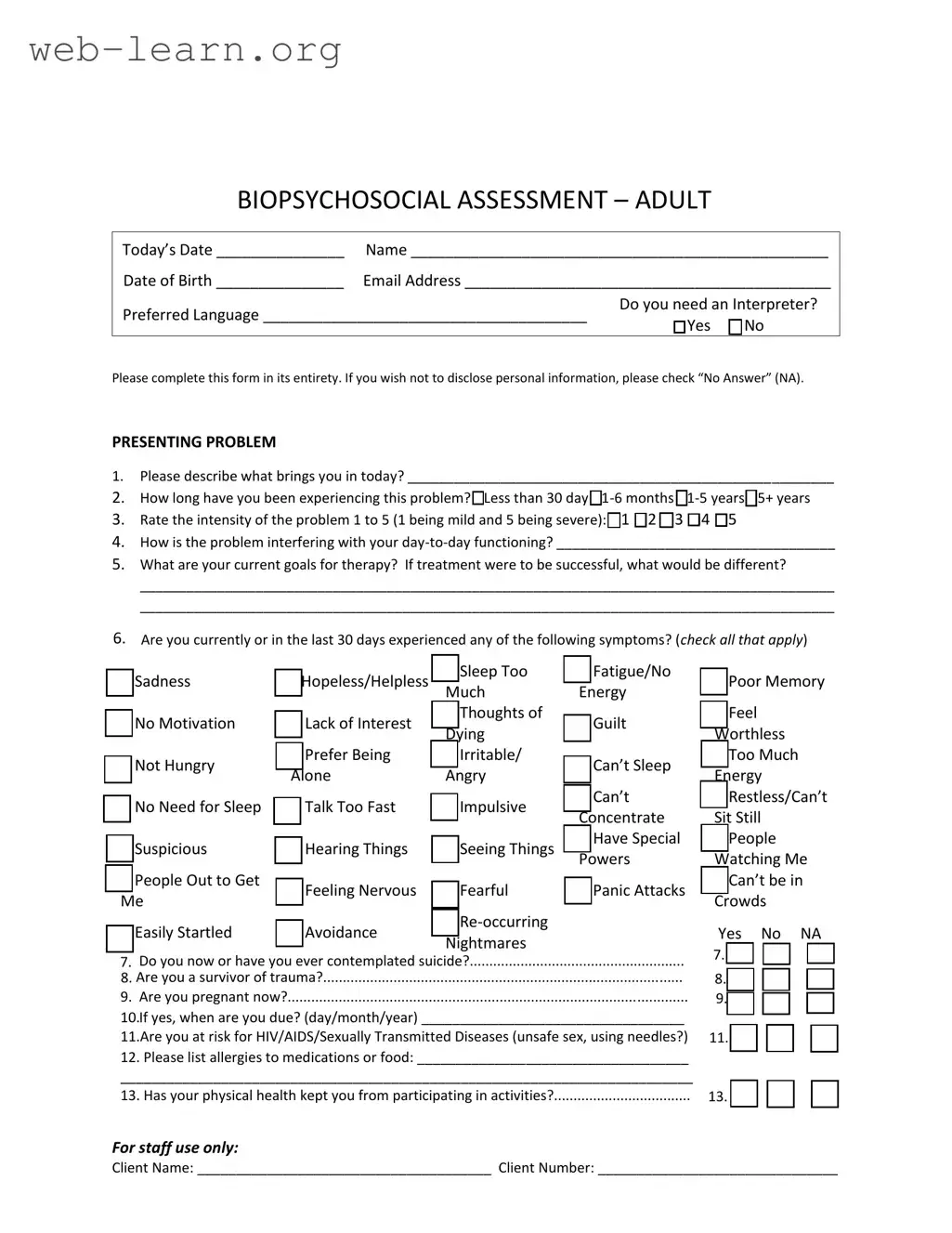
The Biopsychosocial Assessment Social Work form serves as a comprehensive tool for understanding an individual's mental health needs by examining various aspects of their life. It encompasses crucial areas such as presenting problems, personal history, and social relationships. The form prompts individuals to describe the issues that led them to seek help, including the duration and intensity of these problems. Additionally, it explores how these challenges affect daily functioning and outlines personal goals for therapy. It also addresses mental health symptoms, trauma history, and substance use, providing a holistic view of the client's situation. Information about family dynamics, education, legal issues, work history, and medical background is gathered to create a well-rounded profile. By collecting this information, social workers can tailor their approach, ensuring that the support provided is both relevant and effective. The form encourages clients to reflect on their experiences, fostering a collaborative environment where healing can begin.

| Fact Name | Description |
|---|---|
| Purpose of the Assessment | The Biopsychosocial Assessment form is designed to gather comprehensive information about an individual's biological, psychological, and social factors that may affect their mental health and overall well-being. |
| Confidentiality | All information provided in the assessment is kept confidential, ensuring that personal details are protected and only shared with authorized personnel involved in the individual's care. |
| Interpreter Services | The form includes a question about the need for an interpreter, highlighting the importance of clear communication in understanding the individual's needs and experiences. |
| State-Specific Regulations | In states like California, the Biopsychosocial Assessment is governed by the California Welfare and Institutions Code, which outlines the legal requirements for mental health assessments. |
| Symptoms Check | The assessment features a checklist for various symptoms, allowing individuals to identify their experiences and providing a clearer picture of their mental health status. |
Completing the Biopsychosocial Assessment Social Work form requires attention to detail and honesty. Each section is designed to gather essential information about your current situation, background, and needs. Follow these steps to ensure the form is filled out accurately and completely.
A Biopsychosocial Assessment is a comprehensive evaluation used in social work to understand an individual's biological, psychological, and social factors that may affect their well-being. This assessment helps professionals identify the client's needs and develop appropriate treatment plans.
This assessment is crucial because it provides a holistic view of the client's life. By examining biological factors (like health issues), psychological aspects (such as mental health), and social influences (like family dynamics), social workers can create tailored interventions that address the root causes of the client's problems.
Clients should be prepared to share a variety of information, including:
The duration of the assessment can vary, but it typically takes about 60 to 90 minutes. This time allows for a thorough exploration of the client's history and current situation.
Clients have the option to check "No Answer" (NA) for any questions they prefer not to disclose. It is essential for clients to feel comfortable, and they should only share what they are willing to discuss.
Yes, the information provided during the assessment is confidential. Social workers are bound by ethical guidelines and legal regulations to protect client privacy. However, there may be exceptions in cases of imminent harm or legal requirements.
After the assessment, the social worker will review the information and collaborate with the client to develop a treatment plan. This plan will outline goals and strategies for addressing the client's needs and may involve referrals to other services if necessary.
Clients have the right to request a copy of their assessment. It is advisable to discuss this with the social worker during the assessment process to understand the procedures for obtaining a copy.
If you have additional questions or concerns, it is best to reach out directly to the social worker or the agency conducting the assessment. They can provide further clarification and support.
Filling out the Biopsychosocial Assessment Social Work form is an important step for individuals seeking support. However, many people make common mistakes that can hinder the effectiveness of the assessment. One major mistake is providing incomplete information. When individuals skip questions or leave sections blank, it can lead to a lack of understanding about their situation. Each question is designed to gather crucial details that help professionals tailor their approach. Ensuring that all sections are filled out completely is essential for a comprehensive assessment.
Another frequent error involves vague responses. When individuals describe their presenting problems or goals for therapy, they may use broad terms without elaboration. For example, stating "I feel sad" does not convey the full extent of the issue. Instead, providing specific examples and context can greatly enhance the understanding of one’s emotional state. Clear communication allows social workers to better address the underlying issues and develop effective treatment plans.
Some individuals also underestimate the importance of honesty. When answering questions about substance use, mental health symptoms, or past trauma, being truthful is critical. If someone downplays their experiences or omits details due to fear of judgment, it can lead to inadequate support. Social workers are trained to handle sensitive information with care, and honesty fosters a trusting relationship that is vital for effective therapy.
Another mistake is failing to consider the impact of relationships and support systems. Many people overlook the significance of family dynamics or friendships when filling out the form. Relationships can profoundly affect mental health, yet individuals might not fully articulate these connections. By recognizing and describing their social networks, clients can provide social workers with the context needed to understand their challenges better.
Additionally, neglecting to update information can pose challenges. Life circumstances change, and so do personal situations. If someone has experienced a significant life event, such as a job loss or a new relationship, it’s important to reflect these changes on the assessment form. This updated information can be crucial for social workers to provide relevant support and resources.
Finally, many individuals rush through the form, treating it as a mere formality rather than a vital part of their therapeutic journey. Taking the time to thoughtfully consider each question can lead to more meaningful insights. A thorough and reflective approach not only benefits the individual but also enhances the effectiveness of the assessment process as a whole.
The Biopsychosocial Assessment Social Work form is a comprehensive tool that gathers essential information about an individual’s mental, physical, and social well-being. It serves as a foundation for understanding a client’s unique situation and guiding appropriate interventions. Alongside this form, several other documents are commonly utilized to provide a more complete picture of a client’s needs and circumstances. Below are four key forms often used in conjunction with the Biopsychosocial Assessment.
Utilizing these documents alongside the Biopsychosocial Assessment enhances the understanding of a client’s multifaceted needs. Each form plays a distinct role in the overall process of assessment, treatment planning, and ongoing support, ultimately contributing to better outcomes for clients.
The Biopsychosocial Assessment Social Work form is an essential tool for understanding a person's life from multiple perspectives. It helps professionals gather comprehensive information about an individual’s biological, psychological, and social factors. Several other documents share similarities with this assessment form. Here’s a look at six of them:
Each of these documents plays a vital role in helping professionals provide the best care possible. They all work together to paint a complete picture of a client’s life and inform effective interventions.
When filling out the Biopsychosocial Assessment Social Work form, it is important to approach the task thoughtfully. Here are some guidelines to consider:
There are several misconceptions surrounding the Biopsychosocial Assessment Social Work form. Understanding these can help you approach the assessment with clarity and confidence. Here are six common misconceptions:
By dispelling these misconceptions, individuals can approach the Biopsychosocial Assessment with a clearer understanding of its purpose and benefits. This can lead to a more productive experience in the therapeutic process.
Key Takeaways for Filling Out the Biopsychosocial Assessment Social Work Form: