The BCA 12.45 Illinois form plays a crucial role for businesses navigating the complexities of corporate status in the state. This form is primarily used for corporations that wish to dissolve or reinstate their business entities. It serves as an official notification to the Illinois Secretary of State about a corporation's intention, whether to officially dissolve or to reinstate a previously dissolved corporation. Key elements of the form include the corporation's name, the date of dissolution or reinstatement, and the registered agent's information. Additionally, it requires the signature of an authorized representative, ensuring that the request is legitimate and properly documented. Filing this form is essential to maintain compliance with state regulations and to avoid potential penalties. Understanding the nuances of the BCA 12.45 can help corporations effectively manage their legal standing and avoid unnecessary complications.


| Fact Name | Description |
|---|---|
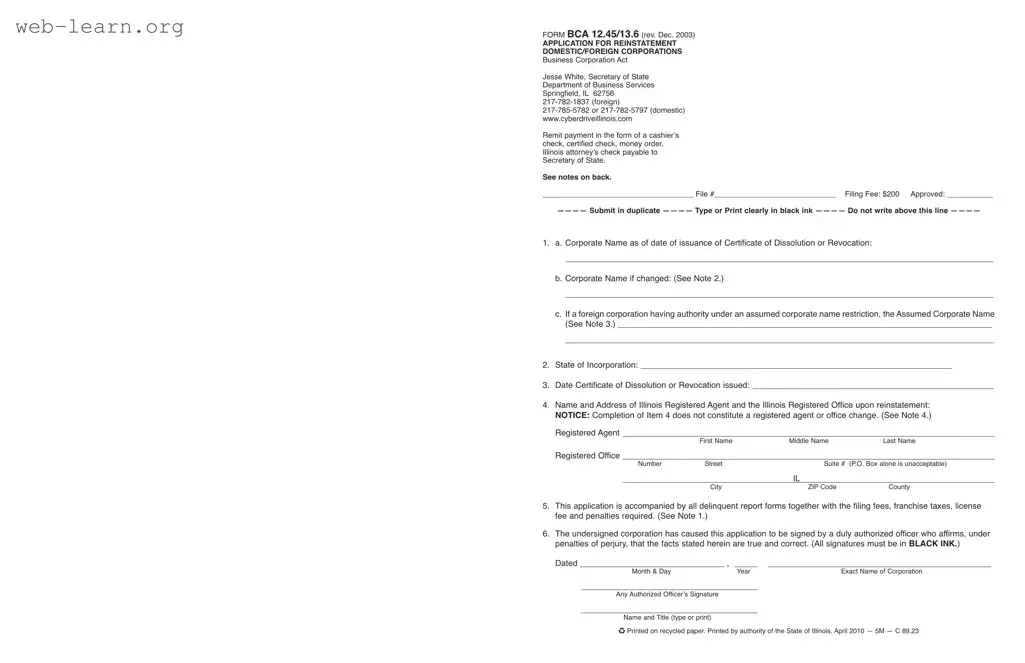
| Form Purpose | The BCA 12.45 form is used to file for the dissolution or reinstatement of a corporation in Illinois. |
| Governing Law | This form is governed by the Illinois Business Corporation Act (805 ILCS 5). |
| Filing Fees | Filing fees are required when submitting the BCA 12.45 form. Fees may vary based on the type of filing. |
| Signature Requirement | The form must be signed by an authorized officer of the corporation to validate the submission. |
| Submission Location | Completed forms should be submitted to the Illinois Secretary of State's office for processing. |
Filling out the BCA 12.45 form in Illinois is an essential step for businesses undergoing specific changes. After completing the form, it should be submitted to the appropriate state department along with any required fees. This process ensures that the changes are officially recognized and recorded.
What is the BCA 12.45 Illinois form?
The BCA 12.45 form is used in Illinois for the dissolution or reinstatement of a corporation. It is essential for businesses that wish to formally end their operations or restore their status after being dissolved.
Who needs to file this form?
This form is necessary for any corporation that has been dissolved and wishes to reinstate its status, or for those that have completed their operations and wish to formally dissolve their business entity.
What information is required on the form?
The form requires details such as:
Are there any fees associated with filing the BCA 12.45 form?
Yes, there are filing fees that must be paid when submitting the form. These fees vary depending on the nature of the filing and any applicable penalties for late submissions.
How long does it take to process the form?
The processing time for the BCA 12.45 form can vary. Typically, it may take several weeks for the Illinois Secretary of State’s office to process the filing, depending on their current workload.
What happens if I do not file this form?
If a corporation fails to file the BCA 12.45 form for dissolution or reinstatement, it may face ongoing penalties and fees. Additionally, the business will remain in a dissolved status, which can affect its ability to conduct future business legally.
Can I file this form online?
Yes, the BCA 12.45 form can typically be filed online through the Illinois Secretary of State’s website. This option can expedite the process and is often more convenient for many businesses.
When individuals or businesses set out to complete the BCA 12.45 form in Illinois, several common pitfalls can lead to complications. One significant mistake is failing to provide the correct corporate name as it appears on the certificate of dissolution or reinstatement. This is critical because any discrepancy can result in delays or even rejection of the application. It is essential to double-check the name against official documents to ensure accuracy.
Another frequent error involves neglecting to include the date of the certificate of dissolution or reinstatement. This date is a vital piece of information that helps establish the timeline of the corporation's status. Omitting this detail can create confusion and may require additional steps to rectify, ultimately prolonging the process.
Individuals often overlook the importance of the registered agent's name and address. This information must be current and accurately filled out. If the registered agent is not properly listed, it can lead to legal complications, as the registered agent is the designated point of contact for any official correspondence. Ensuring that this information is correct is not just a formality; it is a legal requirement.
Additionally, applicants sometimes forget to sign the form. A missing signature can render the entire application void. This oversight may seem minor, but it can cause significant delays in processing. It is advisable to review the form thoroughly before submission to confirm that all required signatures are present.
Lastly, failing to pay the appropriate filing fees is a critical mistake that many make. The BCA 12.45 form requires specific fees that vary depending on the nature of the filing. Not including the correct payment can result in the application being returned or rejected, further complicating the reinstatement or dissolution process. Always verify the fee structure and ensure that payment is included with the submission.
The BCA 12.45 Illinois form is an important document used in the process of business dissolution or reinstatement in the state of Illinois. Alongside this form, several other documents may be necessary to complete your filing. Below is a list of these forms and a brief description of each.
Each of these documents plays a crucial role in the lifecycle of a corporation in Illinois. It is important to ensure that all necessary forms are completed accurately to avoid delays in processing your request. Taking the time to understand these requirements can help facilitate a smoother experience during the dissolution or reinstatement process.
The BCA 12.45 Illinois form is essential for business entities in Illinois, particularly when dealing with the dissolution or reinstatement of corporations. Several other documents serve similar purposes in the realm of business operations and compliance. Here are eight documents that share similarities with the BCA 12.45 form:
Understanding these documents can help business owners navigate the complexities of corporate compliance and ensure that their entities remain in good standing with state regulations.
When filling out the BCA 12.45 Illinois form, it is important to follow certain guidelines to ensure accuracy and compliance. Here are five things to do and five things to avoid:
Misconceptions about the BCA 12.45 Illinois form can lead to confusion for those who need to use it. Here are six common misconceptions, along with clarifications:
Understanding these misconceptions can help ensure that you complete the BCA 12.45 form correctly and avoid unnecessary complications.
Here are key takeaways regarding the BCA 12.45 Illinois form: