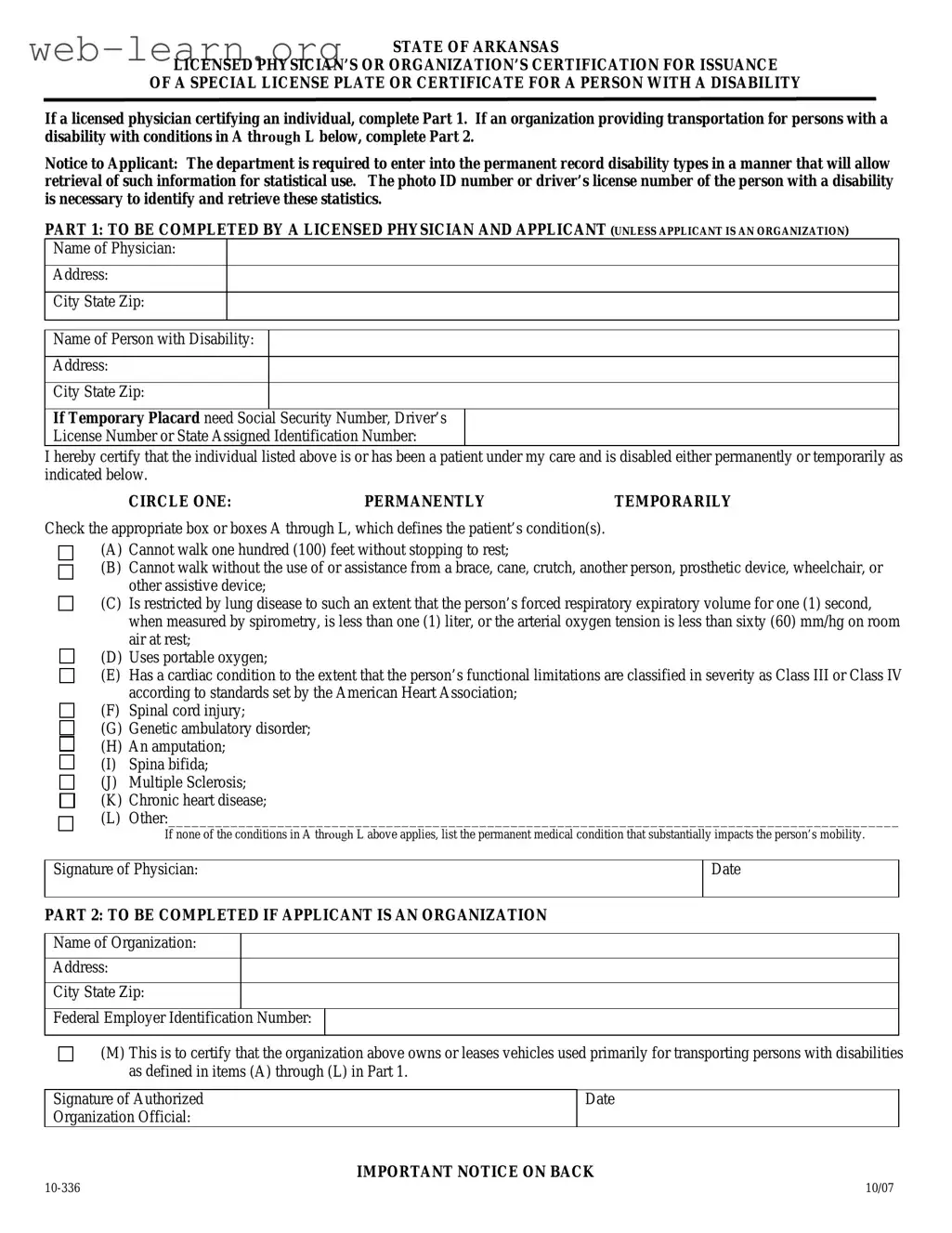
The Arkansas 10 336 form serves as a vital tool for individuals with disabilities seeking special license plates or certificates that facilitate easier access to transportation. This form is divided into two main parts: one for licensed physicians to certify an individual’s disability and another for organizations that provide transportation for persons with disabilities. For physicians, the form requires essential details such as the patient's name and address, along with a certification that the individual is disabled, either temporarily or permanently. The physician must also specify the nature of the disability by selecting from a list of conditions that affect mobility. Organizations, on the other hand, must provide their details and confirm that they operate vehicles primarily used for transporting individuals with disabilities. Additionally, the form emphasizes the importance of accurate information, as misuse or false claims can lead to serious legal consequences. By completing the Arkansas 10 336 form, individuals and organizations can help ensure that those with disabilities receive the support and accommodations they need for safe and accessible transportation.
| Fact Name | Details |
|---|---|
| Purpose of Form | The Arkansas 10 336 form certifies the eligibility of individuals with disabilities for special license plates or certificates, facilitating access to parking and transportation. |
| Governing Law | This form operates under Ark. Code Ann. §27-15-307(7), which outlines the requirements and privileges associated with special license plates for persons with disabilities. |
| Certification Process | Part 1 must be completed by a licensed physician for individuals, while Part 2 is for organizations that provide transportation for persons with disabilities. |
| Expiration of Certificates | The special certificate for permanently disabled individuals expires four years after issuance, while temporary certificates are valid for three months. |
Filling out the Arkansas 10 336 form is an important step in obtaining a special license plate or certificate for individuals with disabilities. The process requires specific information about the individual or organization applying for the certification. Below are the steps to complete the form accurately.
After submitting the form, you will receive further instructions or notifications regarding the status of your application. It is essential to keep a copy of the completed form for your records. If additional information is required, the department will reach out to you directly.
What is the purpose of the Arkansas 10 336 form?
The Arkansas 10 336 form serves as a certification for individuals with disabilities to obtain a special license plate or certificate. This document can be completed by a licensed physician or an organization that provides transportation for persons with disabilities. It helps identify individuals who require special parking privileges due to their mobility challenges.
Who is eligible to complete Part 1 of the form?
Part 1 of the Arkansas 10 336 form must be completed by a licensed physician who is certifying an individual with a disability. The physician must have a valid relationship with the patient and be able to confirm their disability status, whether permanent or temporary.
What information is required in Part 1?
In Part 1, the physician must provide their name, address, and the name and address of the person with a disability. Additionally, the physician must indicate whether the disability is permanent or temporary, and check the relevant boxes that describe the patient's condition from a provided list.
What conditions qualify for a special license plate or certificate?
The form includes a list of conditions that qualify for a special license plate or certificate. These include, but are not limited to:
If none of the listed conditions apply, the physician can specify another permanent medical condition that substantially impacts mobility.
What should an organization do to complete Part 2 of the form?
If the applicant is an organization, Part 2 must be completed. The organization must provide its name, address, and Federal Employer Identification Number. The authorized official must certify that the organization owns or leases vehicles primarily used for transporting persons with disabilities as defined in Part 1.
What are the consequences of providing false information on the form?
Providing false information to obtain a special license plate or certificate is a serious offense. Individuals found guilty of this act may face a Class A misdemeanor charge. This applies to both the person providing false information and those assisting unqualified individuals in acquiring these privileges.
What happens if a special certificate or license plate is no longer needed?
If a person with a special certificate or license plate moves to another state or passes away, they must return the certificate or plate to the nearest Revenue Office. This must be done within a specified time frame, typically within thirty days after the death of the individual.
How long is the special certificate valid?
The special certificate issued for permanently disabled individuals is valid for four years from the last day of the month in which it was issued. For temporary certificates, the validity period is three months. Renewal does not require re-certification of the qualifying disability for permanent certificates.
Completing the Arkansas 10 336 form requires careful attention to detail. One common mistake is failing to provide the correct identification number for the person with a disability. This number, which can be a photo ID number, driver’s license number, or state-assigned identification number, is essential for the department to track disability statistics accurately. Without this information, the application may be delayed or rejected.
Another frequent error involves neglecting to specify whether the disability is permanent or temporary. The form requires the applicant to circle one option, yet some individuals overlook this step. This oversight can lead to confusion and may result in the issuance of an incorrect license plate or certificate.
Inaccurate completion of the medical condition section is also a prevalent issue. Applicants must check the appropriate boxes (A through L) that correspond to the individual’s condition. Failing to check any boxes or selecting the wrong ones can lead to significant complications in the approval process. It is vital that the conditions listed accurately reflect the individual’s health status.
Moreover, signatures are critical. The form requires the signature of the licensed physician or an authorized organization official. Some applicants forget to include this signature, which can render the application invalid. It is important to double-check that all required signatures are present before submission.
Additionally, individuals often overlook the requirement to provide an address for both the physician and the person with a disability. Missing this information can hinder the processing of the application. Ensuring that all addresses are complete and accurate is essential for timely communication from the department.
Lastly, applicants sometimes fail to read the important notices on the back of the form. These notices outline the responsibilities and potential penalties associated with the misuse of the special license plate or certificate. Ignoring this information can lead to unintentional violations of the law, resulting in fines or other legal repercussions.
When applying for a special license plate or certificate for a person with a disability in Arkansas, the Arkansas 10 336 form is essential. However, several other documents may also be required to support your application. Understanding these additional forms can streamline the process and ensure that everything is in order. Below are some common forms and documents that often accompany the Arkansas 10 336 form.
Being prepared with these documents can significantly enhance the efficiency of your application process. Ensuring that all necessary forms are completed accurately and submitted together will help avoid delays and potential complications. Always check with the relevant authorities for any updates or additional requirements that may apply.
The Arkansas 10 336 form serves as a certification for the issuance of special license plates or certificates for individuals with disabilities. Several other documents share similarities with this form in terms of purpose, structure, and the information they require. Below is a list of seven such documents:
When filling out the Arkansas 10 336 form, it is essential to follow specific guidelines to ensure accuracy and compliance. Here is a list of things you should and shouldn't do:
Understanding the Arkansas 10 336 form is crucial for those seeking a special license plate or certificate for persons with disabilities. However, several misconceptions surround this form. Let’s clarify some of these misunderstandings.
This is not true. The form accommodates both permanent and temporary disabilities. Individuals can receive a special certificate even if their disability is temporary, as long as it meets the specified criteria.
In fact, a licensed physician must certify the individual’s disability. This certification is essential for both the applicant and the organization seeking the special plate or certificate.
This is a common misunderstanding. The special plate or certificate is only valid when the vehicle is used to transport the individual for whom it was issued. Misuse can lead to serious penalties.
On the contrary, the special certificate for permanently disabled individuals expires four years after issuance. Temporary certificates expire three months after issuance. Renewal does not require re-certification for permanent disabilities.
When filling out the Arkansas 10 336 form, there are several important points to keep in mind. Understanding these can help ensure a smooth application process for a special license plate or certificate for individuals with disabilities.