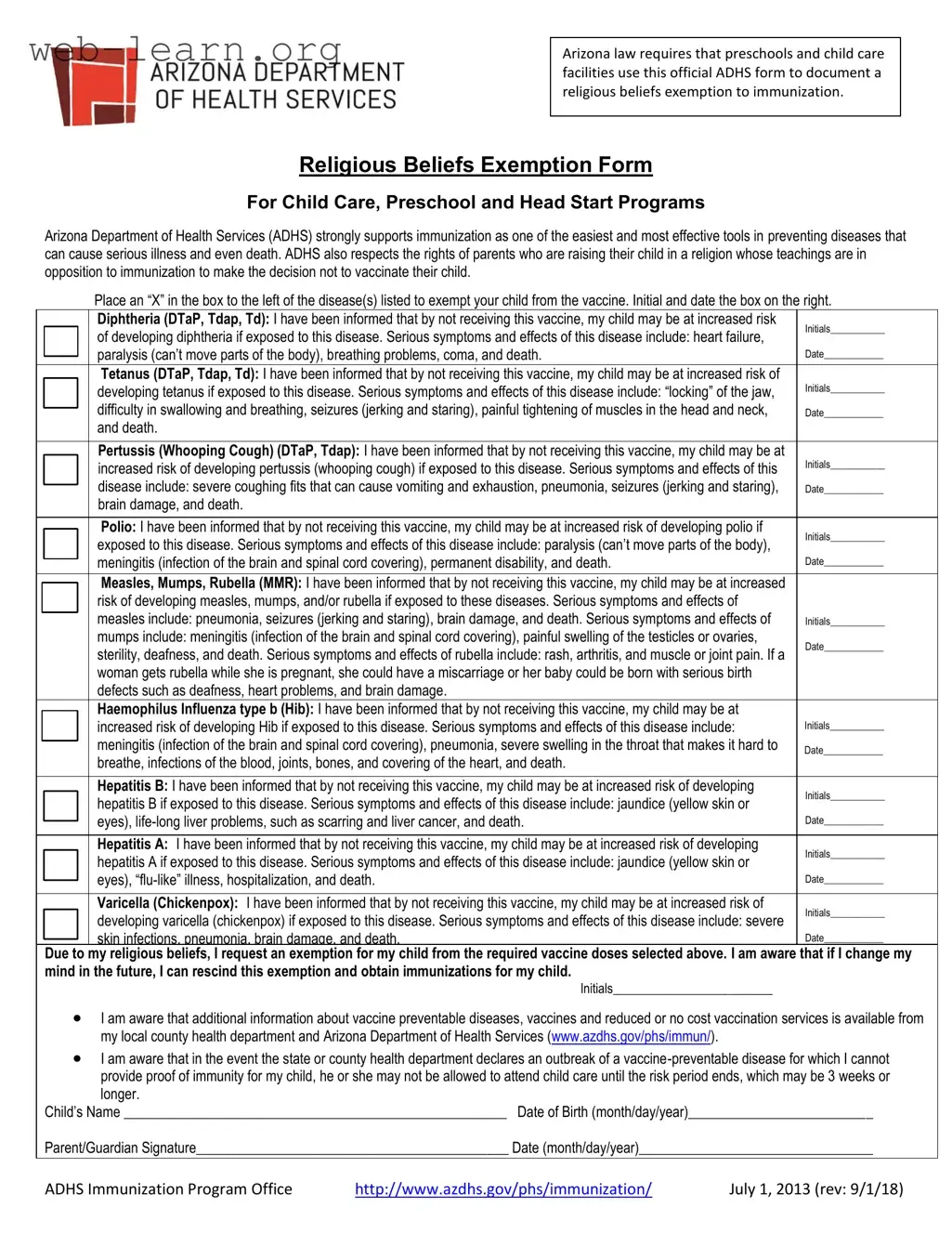
The Arizona Religious Beliefs form is an important document that allows parents to formally request an exemption from immunization requirements for their children based on religious beliefs. This form is mandated by Arizona law for use in preschools and child care facilities. It serves to document the decision of parents who, due to their religious convictions, choose not to vaccinate their children against certain diseases. The Arizona Department of Health Services (ADHS) emphasizes the significance of immunization as a key method for preventing serious illnesses. However, the ADHS also acknowledges the rights of parents to make choices aligned with their religious teachings. The form requires parents to indicate which vaccines they are opting out of by placing an “X” next to the specific diseases listed. Additionally, parents must initial and date next to each vaccine to confirm their understanding of the potential health risks associated with not vaccinating their child. These risks, which are clearly outlined for each disease, include serious health complications such as paralysis, pneumonia, and even death. Furthermore, the form informs parents that they have the option to rescind the exemption in the future should they choose to vaccinate their child. It also notes that during an outbreak of a vaccine-preventable disease, children without proof of immunity may be barred from attending child care facilities until the outbreak risk subsides. Thus, this form plays a crucial role in balancing public health interests with individual rights.
| Fact Name | Details |
|---|---|
| Purpose of the Form | The Arizona Religious Beliefs Exemption Form allows parents to document their religious objections to immunizations for their children in child care, preschool, and Head Start programs. |
| Governing Law | This form is governed by Arizona law, which mandates its use for documenting religious exemptions to immunization requirements. |
| Immunization Support | The Arizona Department of Health Services (ADHS) emphasizes the importance of immunization as a key strategy for preventing serious diseases. |
| Parental Rights | ADHS acknowledges the rights of parents to make vaccination decisions based on their religious beliefs, even if it means opting out of immunizations. |
| Risks of Non-Vaccination | The form includes information on the potential risks associated with not vaccinating, such as increased susceptibility to various diseases and their severe consequences. |
Filling out the Arizona Religious Beliefs form is straightforward. This form is necessary for parents who wish to exempt their child from certain vaccinations based on their religious beliefs. Below are the steps to help you complete the form accurately.
What is the Arizona Religious Beliefs form?
The Arizona Religious Beliefs form is an official document required by Arizona law for parents or guardians who wish to exempt their child from immunizations due to religious beliefs. This form must be used by preschools and child care facilities to document the exemption. It allows parents to formally state their religious opposition to vaccinations while acknowledging the potential health risks associated with not immunizing their child.
How do I fill out the form?
To complete the form, you will need to:
Make sure to review the form carefully before submitting it to ensure all information is accurate and complete.
What happens if I change my mind?
If you decide to rescind the exemption in the future, you can obtain immunizations for your child at any time. It is essential to keep track of your child’s vaccination records and consult with a healthcare provider about the appropriate vaccinations needed.
Are there any consequences for not vaccinating my child?
Yes, if there is an outbreak of a vaccine-preventable disease and you cannot provide proof of immunity, your child may not be allowed to attend child care or school until the risk period ends. This period can last three weeks or longer, depending on the specific disease outbreak.
Where can I find more information about vaccines?
Additional information regarding vaccine-preventable diseases, vaccines, and low-cost vaccination services is available through your local county health department and the Arizona Department of Health Services. You can visit their website at www.azdhs.gov/phs/immunization/ for more resources and guidance.
Filling out the Arizona Religious Beliefs form can be a straightforward process, but there are several common mistakes that individuals often make. One frequent error is neglecting to place an “X” in the appropriate boxes next to the vaccines they wish to exempt. This step is crucial, as it clearly indicates which immunizations are being declined. Without this clear marking, the form may be considered incomplete, leading to potential delays in processing.
Another common mistake involves failing to provide initials and dates in the required sections. Each vaccine listed on the form has a space for initials and a date, indicating that the parent or guardian has acknowledged the risks associated with not vaccinating. Skipping these sections can result in the form being rejected, as it may appear that the parent did not fully understand the implications of their decision.
Some individuals mistakenly think that they only need to sign the form at the end. However, it is essential to initial and date each section where it is required. This ensures that all information is acknowledged and that the parent is fully aware of the consequences of their choice. Omitting initials in any of these sections can lead to complications in the exemption process.
Another area where mistakes occur is in the child’s name and date of birth section. Parents sometimes write the information incorrectly or forget to fill it out entirely. Providing accurate details is vital, as discrepancies can cause confusion or delays in processing the exemption request.
People may also overlook the importance of the parent or guardian's signature. It’s essential to ensure that the signature matches the name provided on the form. Any mismatch can raise questions and potentially lead to the form being deemed invalid.
Additionally, some parents fail to read the information provided about the risks associated with not vaccinating. This part of the form is not just a formality; it’s a critical component that ensures parents are fully informed. Ignoring this section can lead to misunderstandings about the potential health risks to their child.
Another mistake is not being aware of the implications of an outbreak. The form states that if an outbreak occurs and proof of immunity is not provided, the child may be excluded from child care. Parents should be aware of this risk and consider it when making their decision.
Finally, some individuals do not take the time to review the entire form before submitting it. A thorough review can catch any errors or omissions that might otherwise lead to complications. Taking a few extra minutes to double-check the form can save time and frustration later on.
The Arizona Religious Beliefs form is a crucial document for parents seeking an exemption from immunization requirements for their children in child care and preschool settings. Along with this form, there are several other documents that may be necessary to ensure compliance with state regulations and to provide additional context regarding the exemption process. Below is a list of related forms and documents.
Understanding these documents and their purposes can help streamline the exemption process and ensure that all necessary information is provided. It is essential to stay informed and prepared when navigating immunization requirements for your child.
When filling out the Arizona Religious Beliefs form, it is important to follow certain guidelines to ensure that the process goes smoothly. Here are six things you should and shouldn't do:
Understanding the Arizona Religious Beliefs form is essential for parents considering a religious exemption to immunization. However, several misconceptions may lead to confusion. Below is a list of common misunderstandings regarding this form:
Being informed about these misconceptions can help parents navigate the process with clarity and confidence. It is important to approach the topic with care and understanding, as each family's situation is unique.
When filling out the Arizona Religious Beliefs form, keep these key points in mind: