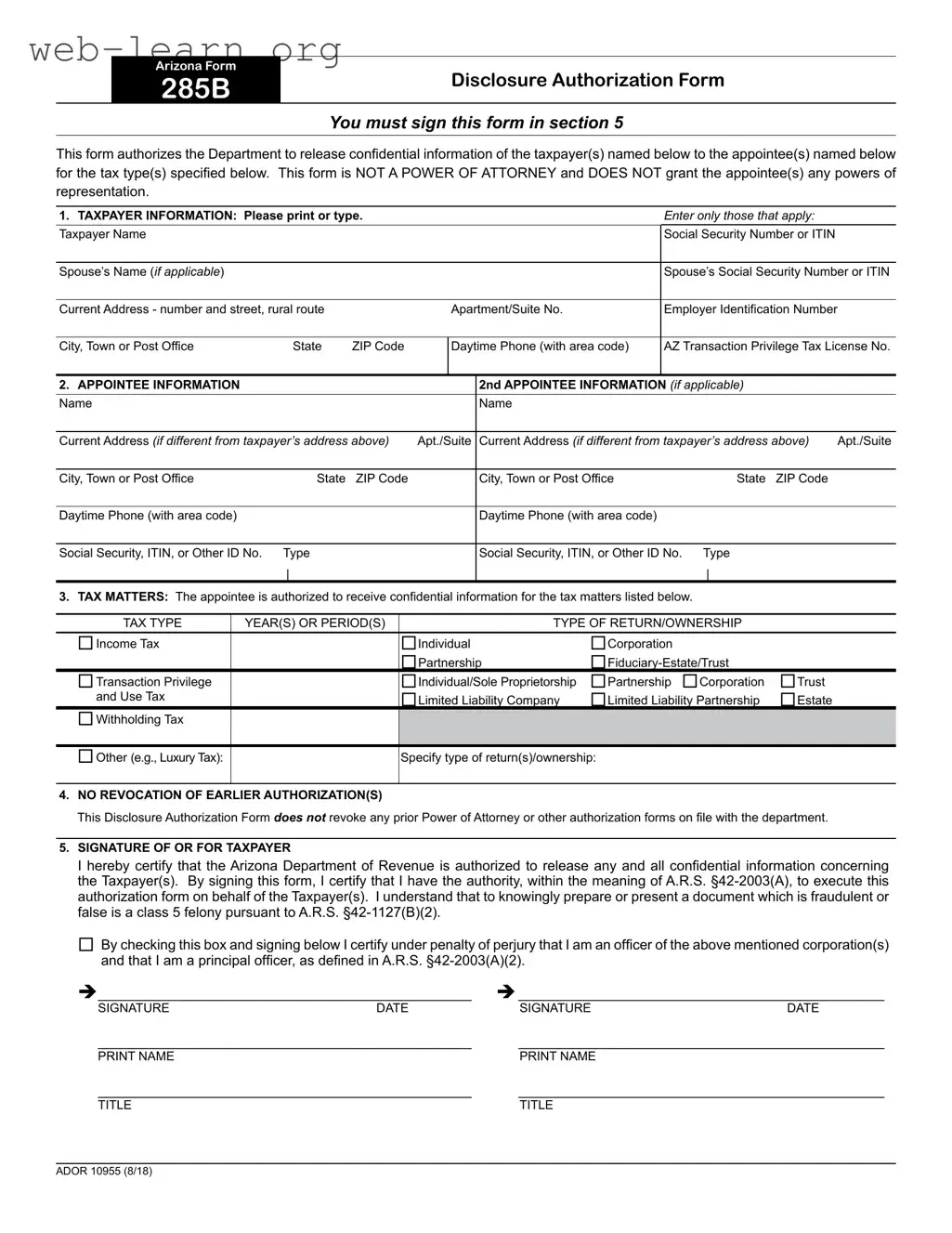
The Arizona 285 form, officially known as the Disclosure Authorization Form, plays a crucial role for taxpayers in the state. This form allows individuals to authorize the Arizona Department of Revenue to share their confidential tax information with designated appointees. It's important to note that this form does not function as a power of attorney; it simply grants access to specific tax details without allowing the appointee to act on behalf of the taxpayer. When filling out the form, taxpayers must provide their personal information, including names, Social Security numbers, and contact details. Additionally, they can specify the appointees who will receive this information, along with the types of tax matters involved, such as income tax or transaction privilege tax. The form also includes a section to confirm that previous authorizations remain valid, ensuring that taxpayers maintain control over their tax representation. Finally, the form requires a signature to certify the accuracy of the information provided and to affirm the authority to execute the authorization.
| Fact Name | Details |
|---|---|
| Form Title | Arizona Form 285B Disclosure Authorization Form |
| Signature Requirement | This form must be signed in section 5 by the taxpayer. |
| Purpose | The form allows the Department to release confidential taxpayer information to designated appointees. |
| Not a Power of Attorney | This form does not grant any powers of representation to the appointee(s). |
| Taxpayer Information | Taxpayer details, including name and Social Security Number or ITIN, must be provided. |
| Appointee Information | Information for one or two appointees can be included, including their contact details. |
| Tax Matters | The appointee can receive information for specific tax types and periods as listed on the form. |
| No Revocation | This form does not revoke any prior Power of Attorney or authorization forms. |
| Governing Law | Relevant Arizona Revised Statutes include A.R.S. §42-2003(A) and A.R.S. §42-1127(B)(2). |
Filling out the Arizona 285 form requires careful attention to detail to ensure that all necessary information is provided accurately. This form allows for the disclosure of confidential taxpayer information to designated appointees. Following the steps below will help ensure that the form is completed correctly.
Once the form is completed, it should be submitted to the appropriate department as instructed on the form. Ensure that all information is accurate and legible to avoid any delays in processing. Keep a copy of the completed form for your records.
What is the purpose of the Arizona 285 form?
The Arizona 285 form, also known as the Disclosure Authorization Form, is used to authorize the Arizona Department of Revenue to release confidential taxpayer information to designated appointees. It is important to note that this form does not grant the appointee any powers of representation, as it is not a Power of Attorney.
Who needs to fill out the Arizona 285 form?
Taxpayers who wish to allow someone else to access their confidential tax information must complete this form. This includes individuals, corporations, partnerships, and other entities that need to designate an appointee for specific tax matters.
What information is required on the form?
Can I designate more than one appointee?
Yes, the Arizona 285 form allows for the designation of a second appointee. If you wish to appoint more than one individual, you must provide their information in the designated section of the form.
Does this form revoke previous authorizations?
No, the Arizona 285 form does not revoke any prior Power of Attorney or other authorization forms that may be on file with the Arizona Department of Revenue. It is essential to maintain any existing authorizations if you still require them.
What happens if I do not sign the form?
Failure to sign the Arizona 285 form will prevent the Department of Revenue from releasing any confidential information to the designated appointee(s). The form must be signed in section 5 for it to be valid.
Is there a penalty for providing false information on this form?
Yes, knowingly preparing or presenting a fraudulent or false document is considered a class 5 felony under Arizona law. It is crucial to provide accurate and truthful information when completing the form.
How can I submit the Arizona 285 form?
The completed Arizona 285 form can be submitted to the Arizona Department of Revenue. It is advisable to keep a copy for your records. Check the Department's website for specific submission instructions, as they may vary based on the method of filing.
When filling out the Arizona 285 form, individuals often make several common mistakes that can lead to delays or complications. One frequent error is failing to sign the form in section 5. This section is crucial, as it authorizes the Department to release confidential information. Without a signature, the form is incomplete and cannot be processed.
Another common mistake involves incorrect taxpayer information. It is essential to ensure that the taxpayer's name, Social Security Number or ITIN, and current address are accurately entered. Any discrepancies can cause issues in verifying identity and may delay processing. Additionally, omitting the spouse’s information when applicable is another oversight that can complicate matters.
People also often neglect to provide complete appointee information. If there is a second appointee, their details must be filled out correctly. Missing information such as the appointee's address or phone number can hinder communication and the overall process. Furthermore, individuals frequently forget to specify the correct tax types and years for which the appointee is authorized to receive information. This section should be filled out carefully to ensure that all relevant tax matters are covered.
Another mistake is misunderstanding the nature of the form itself. The Arizona 285 form is a disclosure authorization and not a power of attorney. Many individuals mistakenly believe that this form grants the appointee powers of representation, which it does not. Clarifying this distinction is vital to avoid confusion.
Additionally, individuals may overlook the section regarding prior authorizations. The form states that it does not revoke any earlier authorizations. Failing to understand this can lead to misunderstandings regarding the authority granted to the appointee.
Lastly, not reviewing the form for accuracy before submission can lead to significant issues. Simple typos or missing information can result in the form being returned or delayed. Taking the time to double-check all entries can prevent these unnecessary complications.
The Arizona 285 form is a Disclosure Authorization Form that allows taxpayers to authorize the release of their confidential information to designated appointees. This form is often used in conjunction with several other documents that facilitate tax-related matters. Below is a list of commonly associated forms and documents.
These documents serve various purposes related to tax reporting, representation, and compliance in Arizona. Each form plays a crucial role in ensuring that taxpayers meet their obligations while allowing for the proper handling of their confidential information.
The Arizona 285 form is used to authorize the release of confidential taxpayer information to designated individuals. It shares similarities with several other documents. Below is a list of eight documents that are similar to the Arizona 285 form, along with a brief explanation of how they are alike:
When filling out the Arizona Form 285, it's essential to approach the task with care. This form is crucial for authorizing the release of confidential tax information. Here’s a list of things you should and shouldn’t do to ensure a smooth process.
Understanding the Arizona Form 285 can be challenging, and several misconceptions often arise. Here are seven common misunderstandings:
Being aware of these misconceptions can help ensure that taxpayers properly navigate the process of using the Arizona Form 285.
Here are some key takeaways about filling out and using the Arizona 285 form: