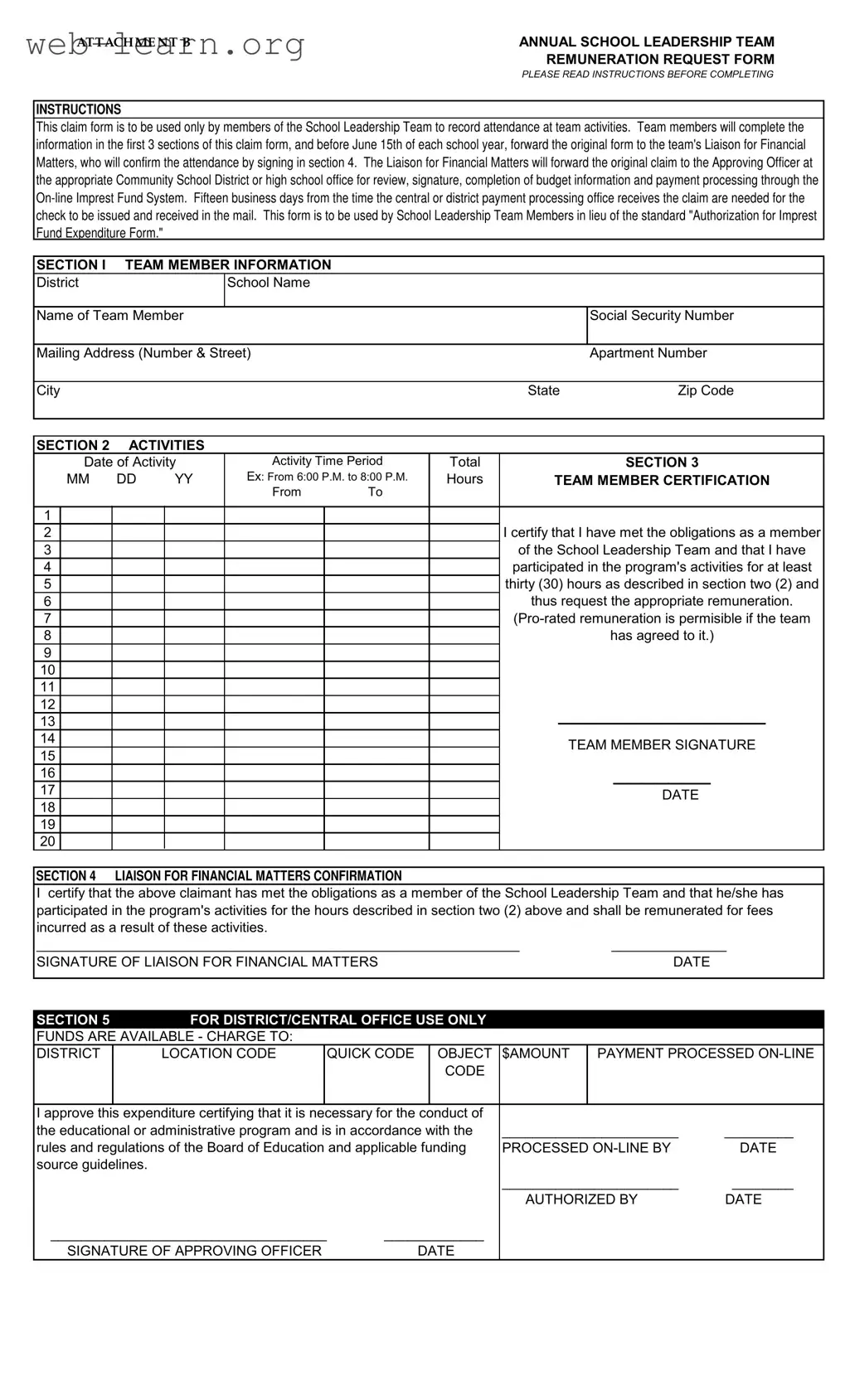
The Annual School Leadership Team Remuneration Request Form serves as a vital tool for members of the School Leadership Team to document their participation in team activities and request appropriate compensation. This form is designed specifically for team members to record their attendance and is divided into several key sections. In the first section, team members provide essential personal information, including their name, mailing address, and Social Security number. The second section focuses on the activities undertaken, requiring members to detail the date, time period, and total hours spent on each activity. Following this, team members must certify their participation, affirming that they have met the required obligations of at least thirty hours of involvement. The form also includes a section for the Liaison for Financial Matters to confirm attendance and authorize remuneration. Finally, the last section is reserved for district or central office use, ensuring that funds are available and the expenditure aligns with educational guidelines. Timely submission is crucial, as members must forward the completed form to the Liaison by June 15th, allowing for adequate processing time for payment through the On-line Imprest Fund System.
| Fact Name | Description |
|---|---|
| Purpose | This form is used by School Leadership Team members to request remuneration for their participation in team activities. |
| Deadline | Members must submit the form by June 15th of each school year. |
| Submission Process | After completion, the original form is sent to the Liaison for Financial Matters for confirmation. |
| Processing Time | It takes fifteen business days for the payment to be processed after the claim is received by the central or district office. |
| Sections | The form consists of five sections, including team member information, activity details, certification, and financial matters confirmation. |
| Pro-rated Remuneration | Pro-rated remuneration is allowed if agreed upon by the team. |
| Governing Laws | This form is governed by the rules and regulations of the Board of Education and applicable funding source guidelines. |
| Use of Form | This form replaces the standard "Authorization for Imprest Fund Expenditure Form" for School Leadership Team members. |
Completing the Annual School Leadership Team form is an important step for team members to receive remuneration for their participation. After filling out the form, it must be submitted to the Liaison for Financial Matters for verification. This process ensures that all necessary approvals are obtained for payment processing.
The Annual School Leadership Team form is designed for members of the School Leadership Team to record their attendance at team activities. This form facilitates the request for remuneration for participation in these activities, ensuring that members are compensated for their time and effort.
This form is exclusively for members of the School Leadership Team. Only those who have participated in the required activities are permitted to complete and submit this form for remuneration.
The form consists of several sections where team members must provide:
Team members must complete the first three sections of the form and submit the original to the Liaison for Financial Matters before June 15th of each school year. The Liaison will then confirm attendance by signing the form and forward it to the appropriate Community School District or high school office.
After the claim is received by the central or district payment processing office, it typically takes fifteen business days for the check to be issued and mailed to the team member.
Yes, pro-rated remuneration is permissible if agreed upon by the team. This allows for flexibility in compensation based on the specific participation of each member.
If there are errors on the form, it is essential to correct them before submission. Inaccuracies may delay processing and payment. Team members should review all sections carefully to ensure that all information is accurate and complete.
The form requires signatures from both the team member and the Liaison for Financial Matters. The Liaison's signature confirms that the member has met the obligations and participated in the required activities.
Filling out the Annual School Leadership Team form can be straightforward, but many individuals still make mistakes that can lead to delays or issues with remuneration. One common error is failing to read the instructions thoroughly before starting. The instructions provide crucial information about how to complete the form accurately. Skipping this step can result in missteps that could have easily been avoided.
Another frequent mistake is not providing complete contact information. Team members often forget to include their full mailing address or may leave out their apartment number. This omission can complicate the payment process, as the school or district office may need to reach out for clarification, causing unnecessary delays.
In section two, many people overlook the importance of accurately recording the dates and times of activities. Incomplete or incorrect entries can lead to confusion about attendance and participation. It’s essential to ensure that all details are precise, as these figures are vital for verifying attendance.
Additionally, some team members may not certify their participation correctly. The certification statement requires a clear acknowledgment of meeting obligations and participation hours. Not filling this out properly can result in the claim being rejected or delayed. Always double-check that this section is completed fully.
Another common issue arises in section four, where the Liaison for Financial Matters must confirm attendance. Sometimes, team members forget to obtain the necessary signature from the Liaison. Without this confirmation, the form cannot proceed to the next stage, which can lead to missed payment deadlines.
Moreover, people often submit their forms after the June 15th deadline. Timeliness is critical in this process. Late submissions can result in not receiving remuneration, as the form must be processed within a specific timeframe. Planning ahead and submitting on time is essential.
Another mistake is not keeping a copy of the submitted form. It’s wise to have a record for personal reference. This can be helpful in case there are any questions or issues later regarding the claim. Not having a copy can leave individuals without proof of their submission.
Lastly, some individuals may fail to follow up on their claims after submission. It’s important to check in with the Liaison for Financial Matters or the district office if payment is delayed. Proactive communication can help resolve any issues that may arise during the processing of the form.
The Annual School Leadership Team form is an essential document for members of the School Leadership Team to request remuneration for their participation in team activities. Several other forms and documents often accompany this form to ensure proper documentation and processing. Below is a list of these related documents.
These documents work together to support the functions of the School Leadership Team, ensuring transparency, accountability, and effective communication. Proper use of these forms will streamline processes and enhance the team's overall performance.
When filling out the Annual School Leadership Team form, there are important guidelines to follow. Here’s a list of what you should and shouldn’t do:
Following these steps will help ensure a smooth process for your remuneration request. Your attention to detail is essential, and it will make a difference in the outcome.
Here are four common misconceptions about the Annual School Leadership Team form:
Filling out the Annual School Leadership Team form correctly is essential for ensuring that team members receive their remuneration promptly. Here are some key takeaways to keep in mind:
By following these guidelines, you can ensure a smooth and efficient process for receiving your remuneration as a valued member of the School Leadership Team.