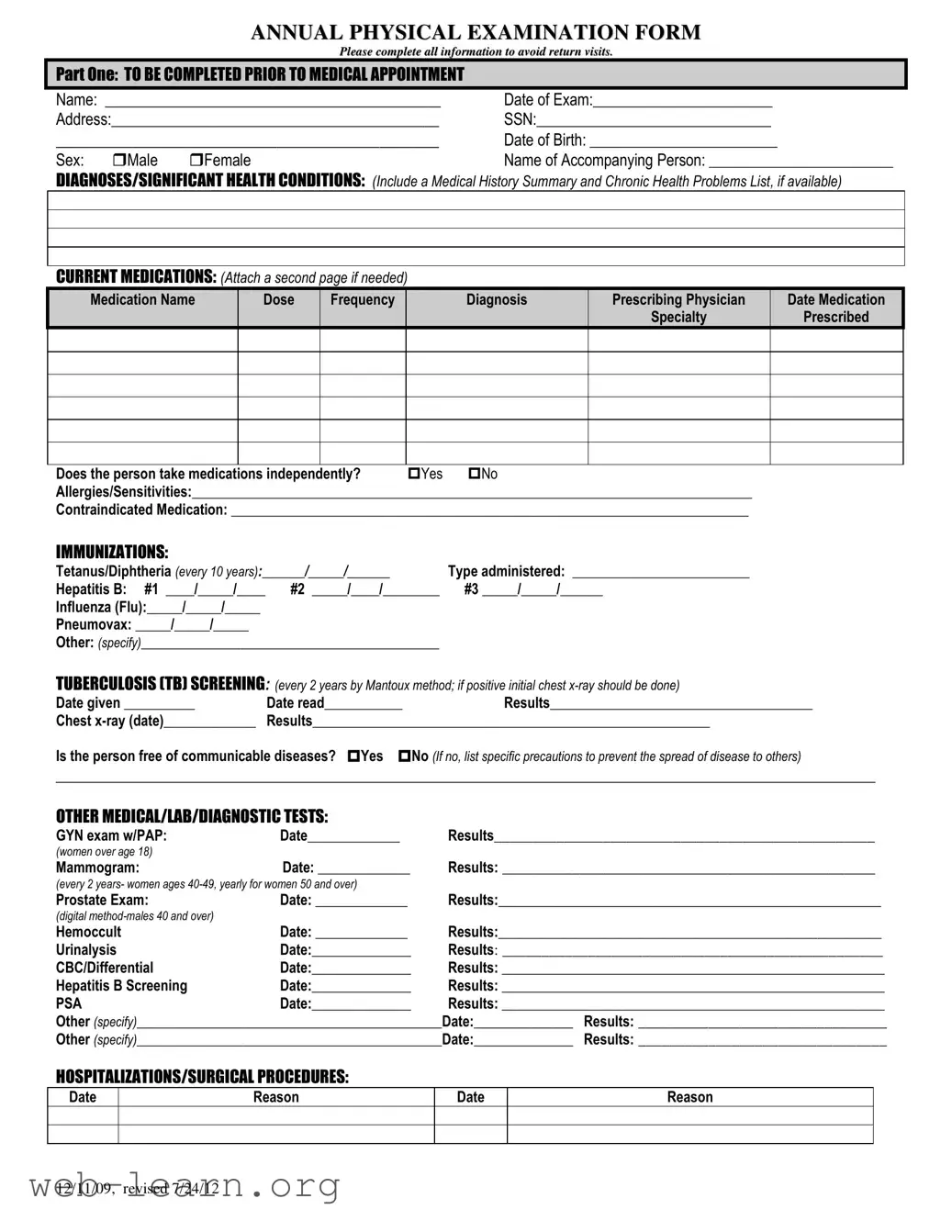
The Annual Physical Examination form serves multiple crucial purposes for both patients and healthcare providers alike. By gathering comprehensive personal information such as the patient's name, date of birth, and contact details, this form establishes a foundational understanding of the individual seeking care. Clinicians can dive deeper into a patient's medical history through sections that request details about diagnoses, significant health conditions, and an overview of current medications. Essential immunization records, including tetanus and flu shots, need to be documented to ensure the patient is adequately protected against preventable diseases. Moreover, it assesses whether any communicable diseases are present, providing an opportunity for proper precautions to mitigate risks. Beyond medical history, the form addresses general physical examination parameters—like blood pressure and heart rate—allowing for an initial snapshot of the individual's health status. Specific tests, including prostate exams for males and mammograms for females, also necessitate documentation to monitor ongoing care. Ultimately, the thorough nature of this form aims to streamline the patient experience and promote effective communication between parties, ensuring that no vital information is overlooked during the examination and subsequent treatments.
| Fact Name | Description |
|---|---|
| Purpose of the Form | The Annual Physical Examination form collects comprehensive health information to support preventive care and address any significant health conditions. |
| Mandatory Information | Sections must include personal details, diagnoses, current medications, allergies, immunizations, and past medical history. |
| Screening Requirements | Includes recommendations for tuberculosis screening every two years and specific exams like GYN and prostate exams based on age and gender. |
| Vaccination Records | Patients must provide dates for crucial vaccines such as Tetanus, Hepatitis B, and Influenza to ensure they are up to date. |
| Legal Considerations | In some states, personal health information is protected under HIPAA and specific state regulations regarding patient confidentiality. |
| Documentation of Medication | Patients should list current medications, prescribing physicians, and any changes made during the appointment for accurate records. |
| Recommendations for Care | The form provides space for doctors to outline health maintenance recommendations, dietary needs, and activity restrictions. |
| Signature Requirement | A physician’s signature and date are required, signifying that the evaluation has taken place and all necessary information has been reviewed. |
Completing the Annual Physical Examination form is essential for ensuring an efficient and thorough medical appointment. Fill out this form accurately to help your healthcare provider better understand your health needs. Follow these steps to complete the form correctly.
What is the purpose of the Annual Physical Examination form?
The Annual Physical Examination form is designed to gather essential health information from patients prior to their medical appointments. Completing the form ensures that healthcare providers have a comprehensive view of a patient's medical history, current medications, allergies, immunizations, and recent health screenings. This documentation aids in accurate diagnosis and tailored treatment plans.
Who should complete the form?
The form should be filled out by the patient or an accompanying individual. It includes personal details like name, address, date of birth, and significant health conditions. Accuracy is critical, as this information directly impacts the quality of care received during the examination.
What specific information is required regarding medications?
Patients must list all current medications, including the name, dosage, frequency, diagnosis, prescribing physician, and any specialty prescribed. If more space is needed, an additional page may be attached. Furthermore, patients should indicate whether they take medications independently and note any allergies or sensitivities.
What immunizations need to be reported?
The form requires details on past immunizations, including Tetanus/Diphtheria, Hepatitis B, Influenza, and Pneumovax, among others. Recording the dates of administration is essential. This data helps healthcare providers determine if booster shots or additional vaccinations are necessary to maintain a patient's immunity.
What should be done if there are significant health changes compared to the previous year?
If there have been health changes, it is imperative to specify these in the designated area of the form. These updates could range from new diagnoses to changes in medication or health status. Noting such changes equips healthcare providers with the most current information, which is vital for ongoing or new treatment plans.
What kind of tests or screenings are included in the physical examination?
The form encompasses various health evaluations such as blood pressure, cardiovascular assessments, visual and hearing screenings, and routine lab tests like CBC and urinalysis. Women may need to report results from GYN exams, while men should provide details about prostate exams. Each of these measures offers insights into different areas of health.
What happens if I do not complete the form fully?
Incomplete forms may result in return visits, as healthcare providers need comprehensive information to conduct thorough evaluations. Missing details can delay diagnosis and treatment, complicating healthcare management. To ensure a smooth appointment, patients are encouraged to fill out all sections of the form accurately.
Completing the Annual Physical Examination form accurately is vital for a smooth medical appointment. However, many individuals make common mistakes that can lead to delays or additional visits. One frequent error is leaving sections of the form incomplete. Essential details like the date of examination or address often get overlooked, which can slow down the office's ability to provide necessary care.
Another mistake is the failure to provide a comprehensive list of current medications. It’s crucial to include prescribing physician, dosage, and frequency for each medication taken. Many people either forget to list certain medications or do not include important information, making it challenging for healthcare providers to understand a patient's prescribing history. This oversight could endanger health if potential drug interactions are not considered.
People also frequently neglect to report allergies and sensitivities. Omitting this critical information can lead to severe consequences during medical treatments. When filling out this form, always ensure that any known allergies are clearly stated to avoid potential reactions to prescribed medications or treatments.
Another area where mistakes occur is in the section concerning communicable diseases. Individuals sometimes check “yes” or “no” without fully considering their health status. Providing accurate information here is essential because it impacts both personal health management and the safety of the surrounding community.
Lastly, many individuals do not take the time to review their responses before submitting the form. This final review is crucial, as it allows for the correction of any inaccuracies. Taking a moment to ensure every section is thorough and correct can save time and ensure a more efficient visit.
When preparing for an annual physical examination, a few additional forms and documents may often be required. Each serves a different purpose and helps in providing a comprehensive view of an individual's health. Here are six commonly used forms that accompany the Annual Physical Examination form:
Having these documents ready during an annual physical examination can streamline the process and ensure a thorough assessment. Proper preparation fosters better communication and enhances the quality of care received.
Patient Information Form: This document collects personal details about the patient, such as name, date of birth, and contact information. Like the Annual Physical Examination form, it ensures the healthcare provider has essential information prior to an appointment.
Medical History Questionnaire: This form gathers information on past medical issues, surgeries, and current health problems. It parallels the Annual Physical Examination by providing a summary of significant health conditions.
Medication List: This document outlines all medications a patient is currently taking, including dosages and prescribing physicians. Similar to the Annual Physical Examination form, it helps avoid medication-related issues during the exam.
Immunization Record: This form details the vaccinations received by the patient. It is akin to the Annual Physical Examination in tracking necessary immunizations during a yearly exam.
Lab Test Requisition Form: Patients use this to request specific laboratory tests. Much like the Annual Physical Examination form, it plays a crucial role in gathering pertinent information for a comprehensive health assessment.
Referral Form: This document is used when a primary care physician refers a patient to a specialist. It shares similarities with the Annual Physical Examination form by detailing the patient’s specific health needs.
Emergency Contact Form: This form includes names and numbers of individuals to call in case of an emergency. It complements the Annual Physical Examination by ensuring that critical information is readily available.
Physical Therapy Evaluation Form: This document assesses a patient’s need for physical therapy services. It is comparable to the Annual Physical Examination form as both evaluate health and wellness requirements.
Health Risk Assessment: This questionnaire identifies potential health risks based on lifestyle and history. Like the Annual Physical Examination form, it aids in developing a personalized care plan for the patient.
Consent for Treatment Form: Patients use this to grant permission for examinations and treatments. It is similar to the Annual Physical Examination form by emphasizing patient involvement in their healthcare decisions.
Misconception 1: An annual physical exam is only for those who feel unwell.
This is not true. Regular physical examinations help monitor your overall health and identify potential issues before they become serious. Even if you feel fine, these exams can catch subtle changes in your health.
Misconception 2: Completing the Annual Physical Examination form is optional.
In fact, filling out the form is essential. The information provided helps your healthcare provider understand your medical history, current medications, and any specific concerns. This ensures a comprehensive evaluation and avoids unnecessary follow-up visits.
Misconception 3: Health insurance always covers annual physical examinations completely.
While many plans offer coverage for annual exams, some may have specific conditions or copayments. It is wise to check with your insurance provider beforehand to understand your coverage and any potential out-of-pocket costs.
Misconception 4: The physical examination form only needs to be completed once.
Each year, you should complete a new form. Your health can change significantly within twelve months, and updated information allows for more accurate assessments and recommendations from your healthcare provider.
Misconception 5: Immunizations and screenings are not necessary if I feel healthy.
This is a common belief, but regular immunizations and screenings are vital for preventative care. They help protect against diseases and detect potential health issues early, which can greatly improve outcomes.
When filling out your Annual Physical Examination form, keep the following key takeaways in mind:
By ensuring all information is accurate and complete, you help facilitate your healthcare experience. Your health is important, and being prepared contributes to a more effective visit.
Do I Need a Bill of Sale If I Have the Title in Oregon - Understanding the legal implications of false statements is crucial when completing this form.
Kansas Open Carry Non Resident - Fingerprinting will occur at the Sheriff’s Office as part of the application process.