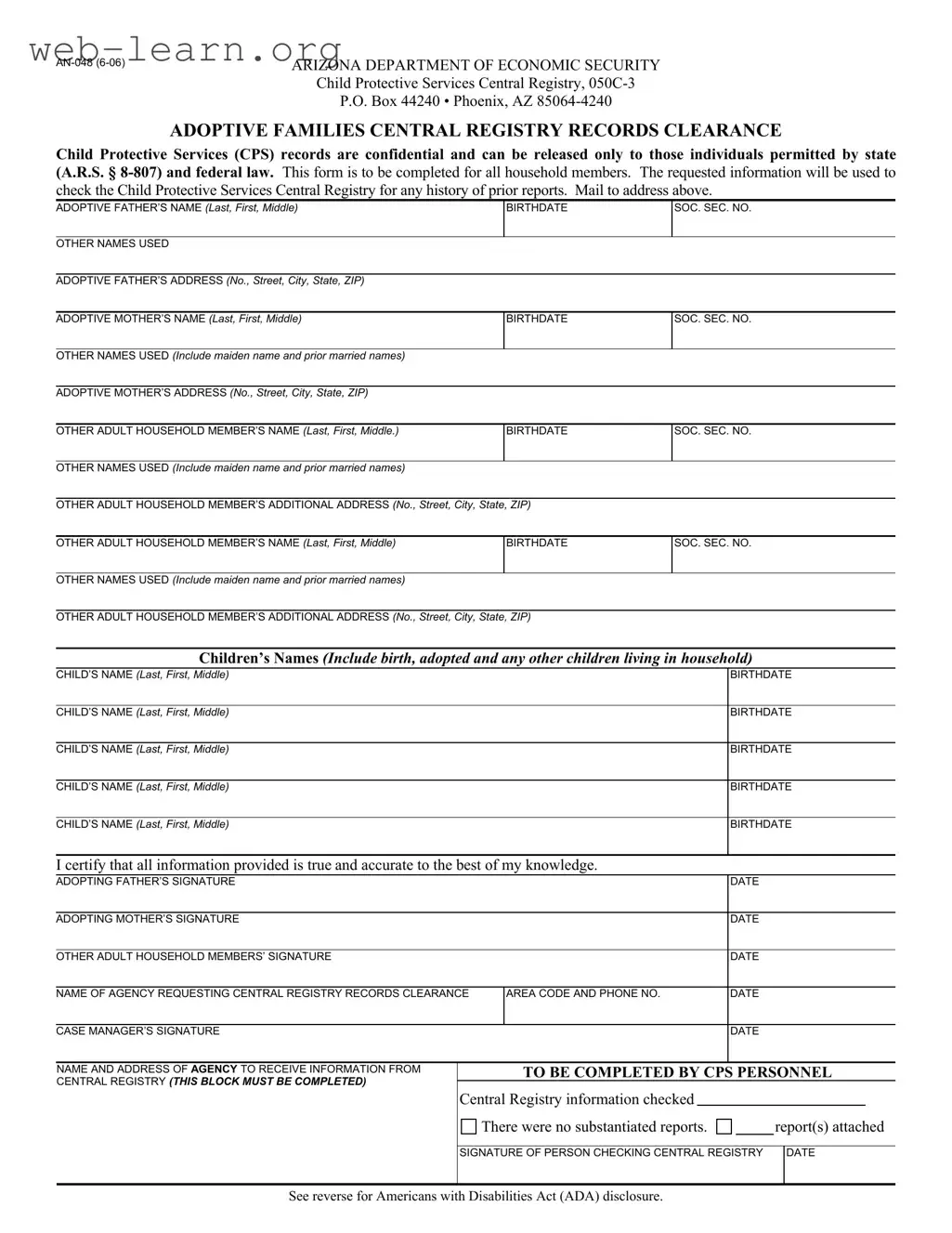
The AN 048 Arizona form plays a crucial role in the adoption process, particularly concerning the safety and well-being of children. This form is essential for adoptive families seeking a clearance from the Child Protective Services (CPS) Central Registry. It ensures that all household members are screened for any history of prior reports, thereby safeguarding the interests of the child being adopted. Completing the form requires detailed information about the adoptive parents and any other adult household members, including their names, birthdates, Social Security numbers, and addresses. Furthermore, it mandates the inclusion of all children living in the household, whether biological or adopted. The information collected is strictly confidential and is only accessible to individuals authorized by state and federal law. After filling out the form, it must be mailed to the designated CPS address for processing. The form also includes a certification statement, where signatories affirm the accuracy of the information provided. This process not only protects children but also upholds the integrity of the adoption system in Arizona.
| Fact Name | Fact Description |
|---|---|
| Form Purpose | This form is used for obtaining a records clearance from the Child Protective Services Central Registry for adoptive families. |
| Confidentiality | Child Protective Services records are confidential and can only be released to individuals permitted by Arizona state law (A.R.S. § 8-807) and federal law. |
| Household Members | The form must be completed for all household members, including adoptive parents and other adults residing in the home. |
| Information Required | Information required includes names, birthdates, Social Security numbers, and addresses of all household members. |
| Children's Information | Details about all children living in the household, including biological and adopted children, must be provided. |
| Signature Requirement | All adopting parents and adult household members must sign the form, certifying that the information provided is accurate. |
| Agency Involvement | The form is often submitted by an agency requesting Central Registry records clearance for the adoptive family. |
| Submission Address | The completed form must be mailed to the Arizona Department of Economic Security at the specified address in Phoenix. |
| ADA Compliance | The form includes a disclosure regarding the Americans with Disabilities Act, ensuring accommodations for individuals with disabilities. |
| Contact Information | For further assistance or to request the form in an alternative format, individuals can contact the provided phone number. |
Completing the AN 048 Arizona form is essential for ensuring that all household members are properly documented for the Child Protective Services Central Registry. This process involves providing accurate personal information for each individual in the household. After filling out the form, you will need to mail it to the specified address for processing.
The AN 048 form is used to request a records clearance from the Child Protective Services (CPS) Central Registry in Arizona. This form must be completed for all adults living in the household of the adoptive family. The information collected is essential for checking any history of prior reports related to child welfare.
All adult household members, including the adoptive father and mother, must complete the AN 048 form. This includes providing personal details such as names, birthdates, Social Security numbers, and any other names used. It is crucial to ensure that all information is accurate and complete to avoid delays in the clearance process.
Once you have filled out the form, you need to mail it to the address provided at the top of the document:
Make sure to send it as soon as possible to avoid any delays in your adoption process.
After submission, CPS personnel will check the Central Registry for any substantiated reports related to the individuals listed on the form. You will receive a response indicating whether there were any reports or if everything is clear. This process is vital for ensuring the safety and well-being of children in adoptive families.
Completing the AN 048 Arizona form is a crucial step in the adoption process, but many applicants make common mistakes that can delay their application. One frequent error is failing to include all household members on the form. The instructions clearly state that information is required for every adult and child living in the household. Omitting any member can lead to complications in the background check process.
Another common mistake involves incorrect or incomplete personal information. Applicants sometimes miswrite names, birthdates, or Social Security numbers. Such inaccuracies can result in significant delays as the authorities may need to verify the correct information before proceeding with the background check.
Some individuals neglect to provide all previous names used, particularly for adoptive mothers who may have maiden names or prior married names. This omission can hinder the thoroughness of the background check, as the agency may not be able to trace all relevant history without complete name information.
In addition, applicants often forget to sign the form. The certification section requires signatures from the adopting father, adopting mother, and any other adult household members. Without these signatures, the form is incomplete and cannot be processed.
Another mistake occurs when applicants fail to include the name of the agency requesting the records clearance. This information is vital for the agency to understand who is initiating the background check and for what purpose. Omitting it can cause unnecessary confusion and delays.
Moreover, some applicants do not provide a valid contact number. A working phone number is essential for any follow-up questions or clarifications that may arise during the review process. Without this information, communication becomes challenging.
Lastly, individuals may overlook the requirement to mail the completed form to the correct address. Sending it to an incorrect location can lead to further delays in the processing of the application. Ensuring that the form is sent to the specified address is a simple yet critical step in avoiding unnecessary complications.
The AN-048 form is a crucial document for prospective adoptive families in Arizona, used to check for any history of prior reports with the Child Protective Services Central Registry. Alongside this form, several other documents may be required to ensure a comprehensive review process. Below is a list of commonly used forms and documents that accompany the AN-048.
Completing the AN-048 form and these accompanying documents is essential for a successful adoption process. Each document plays a significant role in ensuring that the welfare of the child remains the top priority.
The AN-048 form serves as a crucial document in the adoption process in Arizona, particularly for obtaining a records clearance from the Child Protective Services Central Registry. Several other documents share similarities with the AN-048 form, each serving specific functions in the context of family and child welfare. Below are five documents that resemble the AN-048 form, along with explanations of their similarities.
When filling out the AN-048 Arizona form, it's important to follow some guidelines to ensure your application is processed smoothly. Here are four things you should and shouldn't do:
By following these guidelines, you can help ensure that your application is complete and ready for review. This will help speed up the process and reduce any potential delays.
Understanding the AN 048 Arizona form can be challenging, especially with the many misconceptions surrounding it. Here are seven common misunderstandings:
By understanding these misconceptions, individuals can better navigate the adoption process and ensure that they complete the AN 048 form correctly.
When filling out the AN-048 Arizona form for Child Protective Services, keep these key points in mind: