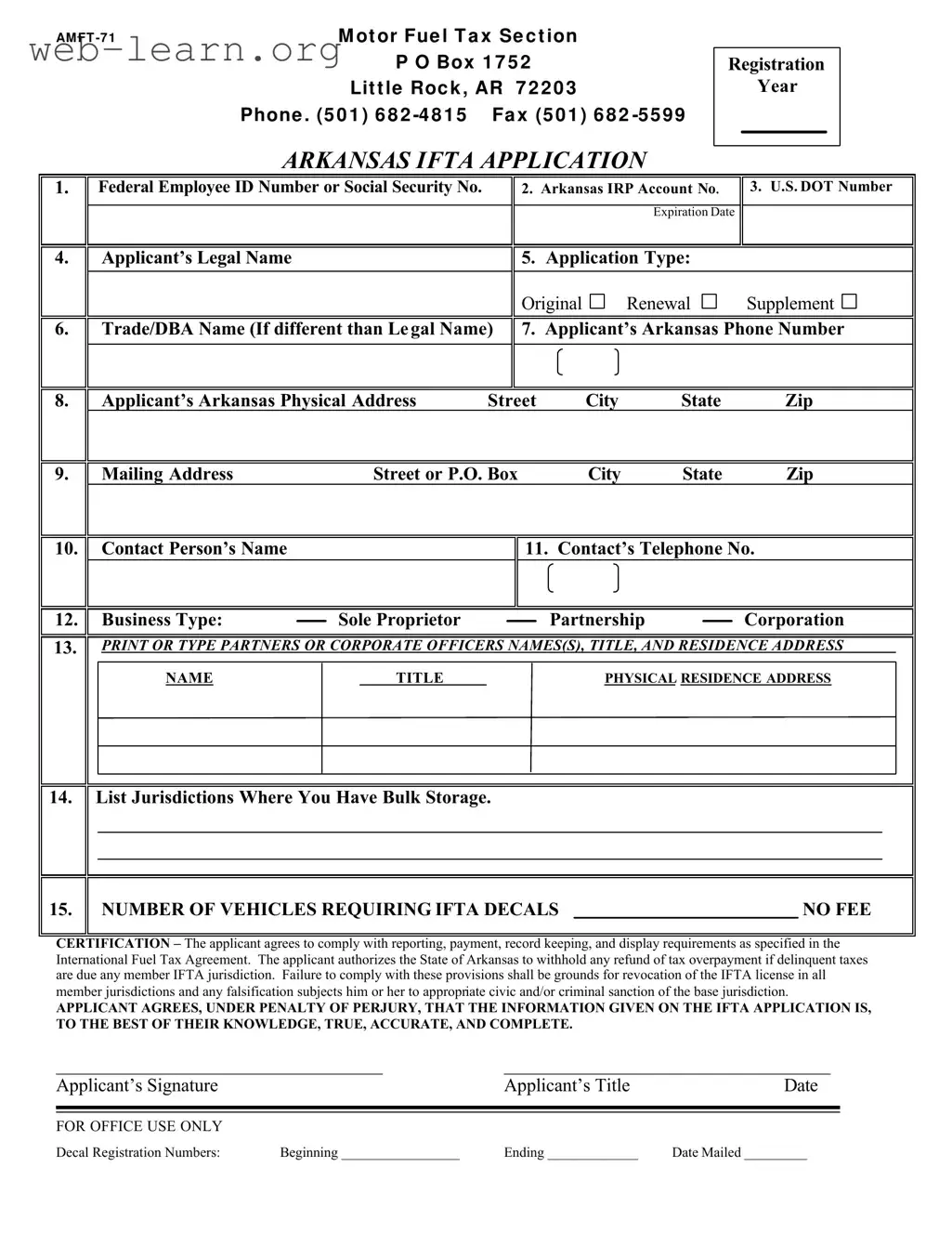
The Amft 71 Arkansas form plays a crucial role for businesses and individuals involved in interstate transportation, specifically for those needing to register under the International Fuel Tax Agreement (IFTA). This form serves as an application for IFTA decals, which are essential for tracking fuel use and tax obligations across state lines. Key components of the form include the applicant's legal name, federal employee ID or social security number, and various identification numbers such as the Arkansas IRP Account and U.S. DOT number. Additionally, the form requires details about the applicant's business type, physical address, and contact information. It also asks for the number of vehicles that will require IFTA decals, which is vital for ensuring compliance with tax regulations. Applicants must affirm their commitment to adhere to reporting and record-keeping requirements, understanding that failure to comply could lead to severe penalties, including the revocation of their IFTA license. The form concludes with a certification statement, where applicants attest to the accuracy of the information provided, underscoring the importance of honesty in this process.
| Fact Name | Details |
|---|---|
| Form Purpose | The AMFT 71 Arkansas form is used for the International Fuel Tax Agreement (IFTA) application, allowing for the reporting of fuel use by motor carriers operating in multiple jurisdictions. |
| Governing Law | This form is governed by the International Fuel Tax Agreement and Arkansas state regulations concerning fuel tax reporting. |
| Contact Information | Applicants must provide their Arkansas phone number and physical address, ensuring that the state can communicate effectively regarding their application. |
| Application Types | The form allows for three types of applications: Original, Renewal, and Supplement, catering to different needs of the applicants. |
| Signature Requirement | Applicants must sign the form, certifying that the information provided is accurate and complete, under penalty of perjury. |
| Vehicle Information | Applicants need to indicate the number of vehicles requiring IFTA decals, which is crucial for proper tax assessment. |
| Delinquency Clause | The form includes a provision that allows the State of Arkansas to withhold tax refunds if there are any delinquent taxes owed in any IFTA jurisdiction. |
Completing the AMFT 71 Arkansas form requires careful attention to detail to ensure all necessary information is accurately provided. Once the form is filled out, it will be submitted to the appropriate state agency for processing. Follow these steps to fill out the form correctly.
What is the purpose of the Amft 71 Arkansas form?
The Amft 71 form is an application for the International Fuel Tax Agreement (IFTA) in Arkansas. This form is essential for businesses that operate commercial vehicles across state lines. It helps ensure that fuel taxes are reported and paid accurately based on the miles driven in each jurisdiction. By completing this form, applicants can obtain the necessary decals for their vehicles, allowing them to comply with fuel tax regulations.
Who needs to fill out the Amft 71 form?
Any business that operates qualifying vehicles in multiple states should complete the Amft 71 form. This includes companies that transport goods or passengers across state lines using vehicles that weigh over a certain threshold, typically 26,000 pounds. It's important for both individual owners and corporations to apply for IFTA decals to ensure compliance with fuel tax laws.
What information is required on the Amft 71 form?
The form requires several key pieces of information, including:
Additionally, the applicant must certify that the information provided is accurate and complete.
What happens if the information on the form is inaccurate?
Providing inaccurate information on the Amft 71 form can lead to serious consequences. If any details are found to be false, the applicant may face penalties, including the revocation of their IFTA license. Furthermore, there may be civic or criminal sanctions imposed by the base jurisdiction. Therefore, it is crucial to ensure that all information is correct before submission.
How can I submit the Amft 71 form?
Once the Amft 71 form is completed, it can be submitted by mail or fax to the Arkansas Motor Fuel Tax Section. The mailing address is provided on the form, and the fax number is (501) 682-5599. Ensure that you keep a copy of the submitted form for your records. If you have any questions during the process, you can contact the office at (501) 682-4815 for assistance.
Filling out the Amft 71 Arkansas form can be straightforward, but many people make common mistakes that can lead to delays or complications. One frequent error is failing to include the Federal Employee ID Number or Social Security Number. This information is crucial for the application to be processed correctly. Without it, the form may be returned or rejected.
Another mistake involves not providing the correct U.S. DOT Number. This number is essential for identifying the applicant's business and ensuring compliance with federal regulations. Double-checking this number before submission can save time and prevent issues down the line.
Many applicants also overlook the importance of accurately filling out their Arkansas IRP Account Number. This number must match the records held by the state. Inaccuracies can lead to complications in the registration process.
When listing the Trade/DBA Name, some people forget to include it if it differs from their legal name. This omission can create confusion and result in additional inquiries from the state. It's best to ensure that all names are clearly stated.
Providing an incomplete or incorrect mailing address is another common mistake. The address must be accurate to ensure that all correspondence and decals are sent to the correct location. Missing or incorrect information can cause delays in receiving important documents.
Additionally, some applicants fail to specify the number of vehicles requiring IFTA decals. This information is critical for determining the appropriate fees and ensuring compliance with tax regulations. Not including this can lead to complications with tax reporting.
Many people also neglect to include a contact person’s name and telephone number. This information is vital for any follow-up questions or clarifications the state may have regarding the application. Providing a reliable contact can streamline communication and expedite the process.
Another mistake is not signing the application. The applicant's signature is a legal requirement, and without it, the application is incomplete. This simple oversight can result in the application being returned.
Lastly, applicants often fail to read the certification statement carefully. Understanding the implications of the no fee certification is essential. Agreeing to comply with all regulations and acknowledging the penalties for falsification is a serious commitment that should not be overlooked.
The Amft 71 Arkansas form is essential for individuals and businesses involved in interstate transportation. It serves as the application for the International Fuel Tax Agreement (IFTA) and is crucial for compliance with fuel tax regulations. However, several other documents often accompany this form to ensure comprehensive compliance and record-keeping. Below is a list of related documents, each playing a specific role in the process.
Understanding these documents and their purposes can simplify the compliance process for individuals and businesses involved in interstate transportation. Proper record-keeping and timely submissions will help ensure adherence to regulations and avoid potential penalties.
When filling out the AMFT 71 Arkansas form, it's important to be mindful of certain practices to ensure a smooth application process. Here’s a list of things you should and shouldn't do:
Following these guidelines will help ensure that your application is processed efficiently and without unnecessary complications.
Understanding the Amft 71 Arkansas form can be challenging, especially with the various misconceptions surrounding it. Here are five common misunderstandings, clarified for better comprehension:
This is not true. While the form is used for original applications, it also serves those seeking to renew or supplement their existing registrations.
In fact, the form requires either a Federal Employee ID Number or a Social Security Number. This information helps verify the identity of the applicant.
This form is essential for compliance with the International Fuel Tax Agreement (IFTA). Failing to file can result in penalties and revocation of your IFTA license.
This is a misconception. The Amft 71 form applies to any business operating vehicles that travel across state lines, regardless of size.
Changes can be made. If there are updates or corrections needed after submission, applicants can file a supplement to amend the information.
Here are some key takeaways about filling out and using the Amft 71 Arkansas form: