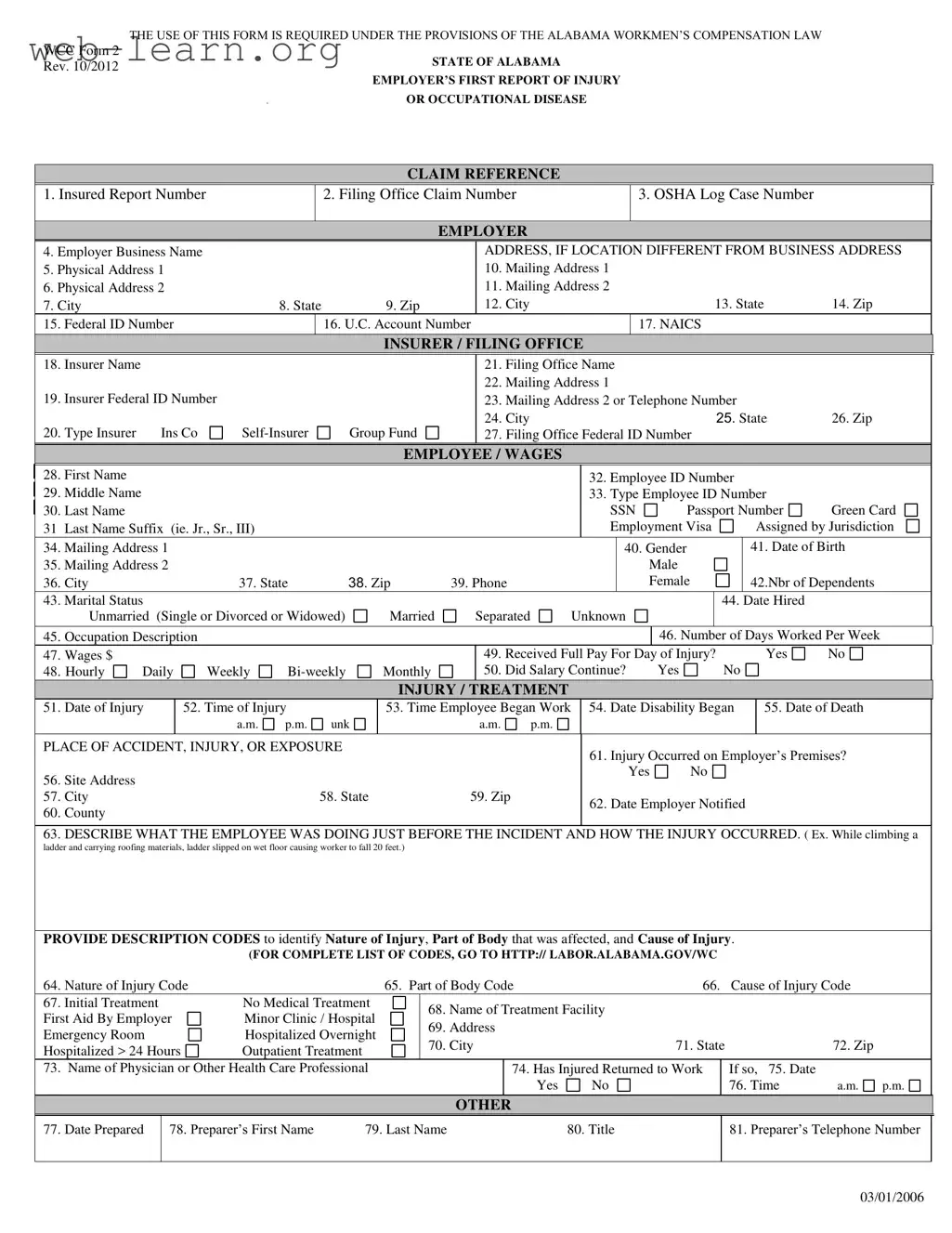
The Alabama First Report form serves a critical role in the state’s workers' compensation system, ensuring that both employers and employees can navigate the process of reporting workplace injuries or occupational diseases effectively. This form is mandated under the Alabama Workmen’s Compensation Law and is essential for documenting various details related to an incident. Key components include information about the employer, such as business name, physical address, and federal ID number, as well as details regarding the employee, including their name, date of birth, and employment status. The form also requires a thorough account of the injury, including the date and time it occurred, the circumstances leading to the incident, and the nature of the injury sustained. Additionally, it captures treatment information and the injured employee's return to work status. By providing a structured approach to reporting, the Alabama First Report form not only facilitates timely claims processing but also promotes the well-being of employees by ensuring that their rights are upheld in the event of a workplace injury.
| Fact Name | Details |
|---|---|
| Governing Law | The Alabama First Report form is governed by the Alabama Workmen’s Compensation Law. |
| Required Use | This form must be used by employers to report injuries or occupational diseases in the workplace. |
| Form Version | The current version of the form is WCC Form 2, revised in October 2012. |
| Employer Information | Employers are required to provide their business name, physical address, and federal ID number. |
| Employee Details | Critical employee information includes name, date of birth, and employment status. |
| Injury Reporting | The form requires detailed descriptions of the injury, including the nature and cause. |
Completing the Alabama First Report form requires accurate and thorough information about the injury or occupational disease claim. Ensure all fields are filled out correctly to facilitate the processing of the claim.
What is the Alabama First Report form?
The Alabama First Report form is a document required under the Alabama Workmen’s Compensation Law. It must be completed by employers to report any work-related injuries or occupational diseases involving their employees. This form helps ensure that injured workers receive the necessary benefits and medical care.
Who is required to file the Alabama First Report form?
Employers in Alabama are required to file this form whenever an employee suffers a work-related injury or illness. This includes both insured employers and self-insured employers. Timely reporting is crucial to facilitate the claims process for the injured worker.
What information is needed to complete the form?
The form requires various pieces of information, including:
How soon must the form be filed after an injury occurs?
The Alabama First Report form should be filed as soon as possible after the injury occurs, ideally within 5 days. Prompt reporting helps ensure that the injured employee receives the necessary benefits without unnecessary delays.
Where can I find the codes for nature of injury, part of body affected, and cause of injury?
A complete list of codes is available on the Alabama Department of Labor's website. You can visit http://labor.alabama.gov/wc to access this information. Using the correct codes is essential for accurate reporting.
What happens if the form is not filed?
Failing to file the Alabama First Report form can lead to delays in benefits for the injured employee. It may also result in penalties for the employer, including fines or increased scrutiny from the Alabama Department of Labor.
Can the injured employee return to work before the form is filed?
Yes, an injured employee may return to work before the form is filed. However, it is important that the employer submits the report promptly to ensure that any necessary workers' compensation benefits are processed without delay.
What should I do if I need assistance completing the form?
If you need help with the Alabama First Report form, consider reaching out to a workers' compensation attorney or a human resources professional. They can provide guidance on how to accurately complete the form and ensure compliance with all legal requirements.
Is there a fee associated with filing the Alabama First Report form?
No, there is no fee to file the Alabama First Report form. However, employers should be aware of any potential costs related to workers' compensation insurance and medical treatment for the injured employee.
Filling out the Alabama First Report form can be a straightforward process, but several common mistakes can lead to complications. One frequent error is failing to provide accurate contact information for both the employer and the employee. Missing or incorrect addresses can delay communication and hinder the processing of the claim. It is crucial to ensure that all physical and mailing addresses are complete and correct.
Another common mistake involves the omission of essential identification numbers. The form requires various identifiers, such as the Employer's Federal ID Number and the Employee's Social Security Number. Neglecting to include these numbers can result in significant delays in processing the claim or even denial of benefits. Always double-check that these numbers are correctly entered.
Many individuals also struggle with the description of the injury or incident. Providing vague or incomplete descriptions can lead to confusion and misinterpretation of the event. It is important to describe what the employee was doing before the injury occurred clearly. Specific details about the circumstances can help ensure that the claim is properly understood and processed.
Additionally, some people fail to indicate the correct nature of the injury or the part of the body affected. The form includes specific codes for these categories, and using incorrect or missing codes can complicate the claim. It is advisable to refer to the complete list of codes provided by the Alabama Department of Labor to ensure accuracy.
Another mistake is not documenting the date and time of the injury accurately. This information is critical for establishing the timeline of events and can affect the claim's validity. Ensure that the date and time fields are filled out clearly and correctly to avoid any issues.
Lastly, individuals often overlook the importance of signing and dating the form. A missing signature or date can render the form incomplete and invalid. This simple step is essential to ensure that the report is officially recognized and processed by the appropriate authorities.
The Alabama First Report form is a crucial document for employers to report workplace injuries or occupational diseases. However, it is often accompanied by several other forms and documents that help streamline the claims process and ensure compliance with state regulations. Below is a list of related documents that are frequently used alongside the Alabama First Report form.
Understanding these additional documents is essential for both employers and employees navigating the workers' compensation process in Alabama. Each form plays a significant role in ensuring that claims are handled efficiently and that all parties are informed throughout the process.
The Alabama First Report form is essential for reporting workplace injuries and occupational diseases. It shares similarities with several other documents used in various contexts. Below is a list of documents that are comparable to the Alabama First Report form, highlighting their similarities:
When filling out the Alabama First Report form, it is essential to approach the task with care and attention to detail. Below is a list of things to do and avoid to ensure that your submission is accurate and complete.
Understanding the Alabama First Report form is crucial for both employers and employees involved in workplace injuries. However, several misconceptions can lead to confusion and potential issues in the claims process. Here are four common misconceptions:
Addressing these misconceptions is essential for ensuring that all parties understand their rights and responsibilities. Properly completing and submitting the Alabama First Report form can significantly impact the outcome of a worker's compensation claim.
When filling out the Alabama First Report form, keep these key takeaways in mind:
Following these guidelines will help ensure that the Alabama First Report form is completed correctly and efficiently.