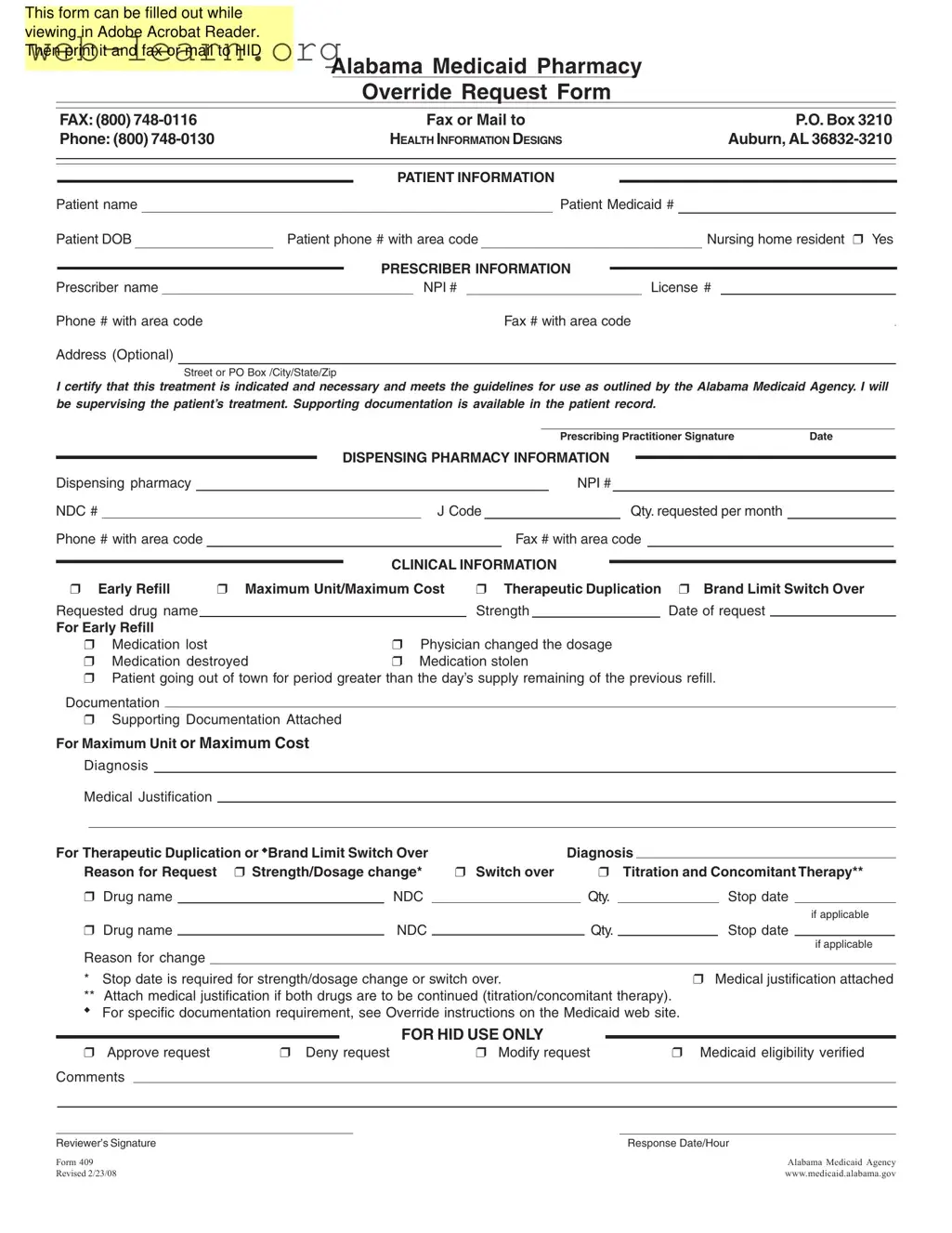
The Alabama 409 form serves as a crucial tool for healthcare providers seeking authorization for specific medication overrides within the Alabama Medicaid system. This form is designed to streamline the process of requesting exceptions to standard medication guidelines, ensuring that patients receive the necessary treatments without unnecessary delays. It can be conveniently filled out using Adobe Acrobat Reader, allowing for easy printing and submission via fax or mail. Key sections of the form include patient and prescriber information, which capture essential details such as names, Medicaid numbers, and contact information. Additionally, the form requires clinical information that supports the request, whether it pertains to early refills, maximum unit limits, or therapeutic duplication. The prescriber must certify the necessity of the treatment, affirming that it aligns with the guidelines set forth by the Alabama Medicaid Agency. By including a section for dispensing pharmacy details and the specific medication being requested, the form ensures that all relevant information is readily available for review. Ultimately, the Alabama 409 form plays a vital role in facilitating timely access to necessary medications for patients in need.
| Fact Name | Description |
|---|---|
| Form Purpose | The Alabama 409 form is used to request pharmacy overrides for Medicaid patients in Alabama. |
| Governing Law | This form is governed by the regulations set forth by the Alabama Medicaid Agency. |
| Submission Method | Completed forms can be faxed or mailed to the designated address provided on the form. |
| Patient Information Required | Information such as the patient's name, Medicaid number, date of birth, and phone number is required. |
| Prescriber Certification | The prescriber must certify that the treatment is necessary and meets Medicaid guidelines. |
| Clinical Information Sections | The form includes sections for early refill requests, maximum unit/cost, therapeutic duplication, and brand limit switch over. |
| Supporting Documentation | Documentation may be required to support the request, especially for specific clinical circumstances. |
Completing the Alabama 409 form is a straightforward process that requires careful attention to detail. Once filled out, the form should be printed and sent via fax or mail to the appropriate address for processing. Below are the steps to accurately complete the form.
What is the Alabama 409 form?
The Alabama 409 form is a request form used for pharmacy overrides in the Alabama Medicaid program. It allows healthcare providers to request exceptions to standard medication coverage rules. This form can be filled out online using Adobe Acrobat Reader, printed, and then submitted via fax or mail.
Who needs to fill out the Alabama 409 form?
The form must be completed by a prescriber, such as a doctor or nurse practitioner, who is supervising the patient's treatment. They will provide necessary patient and prescriber information to support the request.
How do I submit the Alabama 409 form?
Once the form is filled out, it can be submitted either by fax or by mail. The fax number is (800) 748-0116, and the mailing address is:
If you have questions, you can call the Medicaid Pharmacy department at (800) 748-0130.
What information is required on the form?
The form requires various details, including:
What types of requests can be made using the Alabama 409 form?
Requests can be made for several reasons, such as:
Is supporting documentation necessary?
Yes, supporting documentation is often required to justify the request. This documentation should be attached to the form. For specific requirements, refer to the override instructions on the Medicaid website.
What happens after I submit the form?
After submission, the form will be reviewed by the Medicaid Pharmacy department. They will either approve, deny, or modify the request. You will receive a response along with any comments from the reviewer.
Where can I find more information about the Alabama 409 form?
For more details, you can visit the Alabama Medicaid website. They provide comprehensive information about the form and the override process.
Filling out the Alabama 409 form can be straightforward, but many people make common mistakes that can delay the approval process. Understanding these pitfalls can help ensure your request is processed smoothly.
One frequent error is failing to provide complete patient information. Missing details such as the patient's Medicaid number or date of birth can lead to immediate rejection of the request. Always double-check that all fields are filled in accurately before submission.
Another mistake involves the prescriber’s information. Incomplete or incorrect entries, such as an invalid license number or NPI number, can cause significant delays. Ensure that the prescriber’s contact information is current and that all required fields are filled out.
Many people overlook the importance of supporting documentation. If the form indicates that documentation is necessary, be sure to attach it. Failing to include this information can result in a denial of the request.
Additionally, not marking the correct clinical information can lead to confusion. For instance, if you are requesting an early refill, make sure to check the appropriate box and provide a valid reason. Inaccurate selections can derail the entire request.
Some individuals also forget to sign the form. A missing signature can halt the process entirely. Always remember to sign and date the form before sending it off.
Lastly, not following the submission guidelines can lead to complications. Whether faxing or mailing, ensure you have the correct contact information and follow the specified procedures. Inaccurate submissions can result in delays or denials.
By avoiding these common mistakes, you can improve the chances of your request being approved without unnecessary delays. Always take the time to review the form carefully before submitting it.
The Alabama 409 form is crucial for submitting requests related to pharmacy overrides in the Medicaid system. However, several other documents often accompany this form to ensure a comprehensive and effective submission. Below is a list of these additional forms and documents.
Submitting the Alabama 409 form along with these additional documents can streamline the approval process and enhance the likelihood of a successful request. Ensure all information is accurate and complete to avoid delays.
The Alabama 409 form serves as a critical document in the process of requesting pharmacy overrides for Medicaid. Several other forms share similar purposes and structures, often used in healthcare and insurance contexts. Below is a list of documents that are comparable to the Alabama 409 form:
Each of these forms plays a vital role in ensuring that patients receive the necessary medications and services while adhering to regulatory requirements. They all require specific patient and prescriber information, as well as justification for the requests made.
When filling out the Alabama 409 form, it’s important to follow some guidelines to ensure your submission is successful. Here are four things you should and shouldn't do:
Following these tips can help streamline the process and avoid delays in approval. Always double-check your entries before submitting the form.
Here are six common misconceptions about the Alabama 409 form:
When filling out and using the Alabama 409 form, keep these key takeaways in mind: