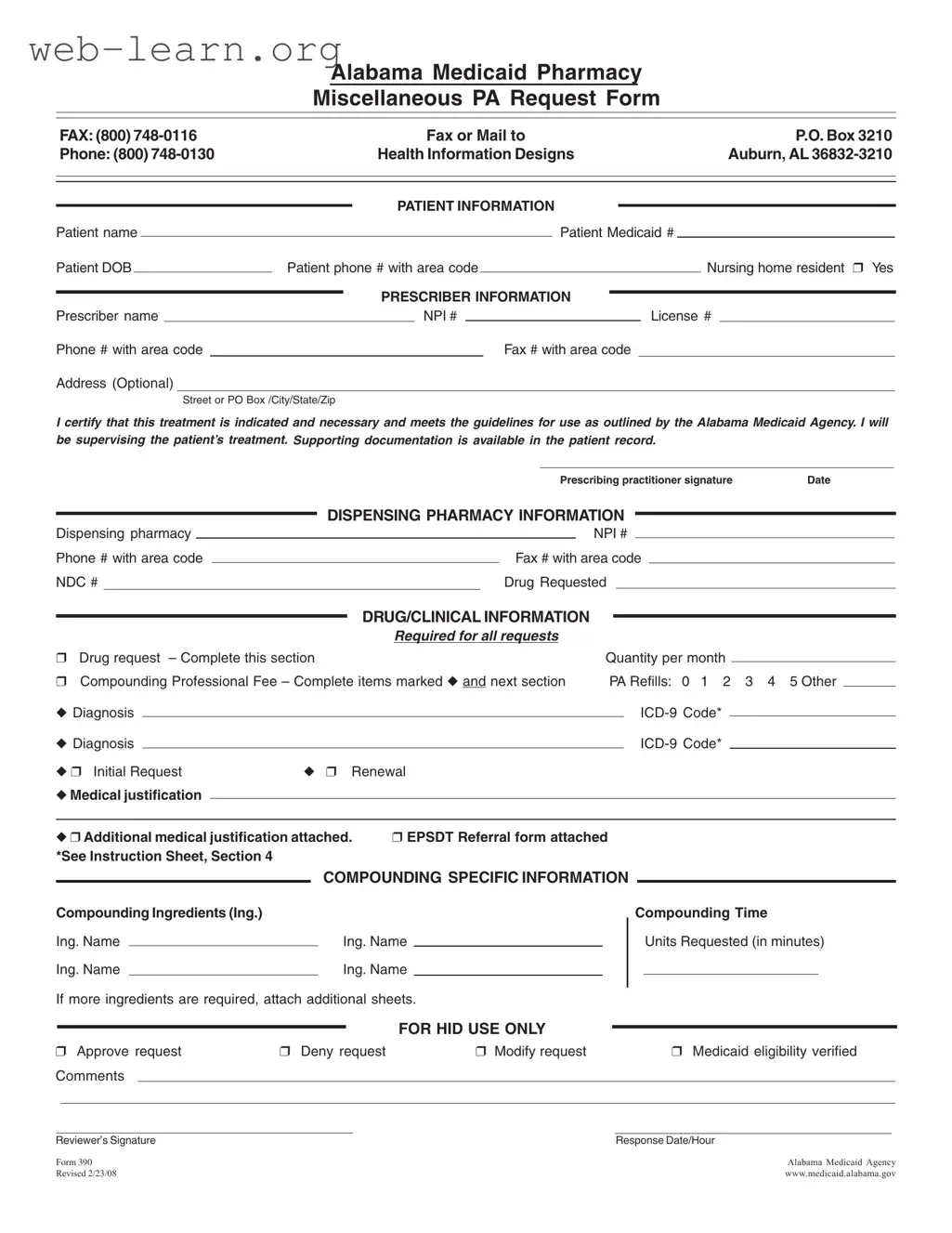
The Alabama 390 form is a crucial document for healthcare providers seeking prior authorization for pharmacy services under the Alabama Medicaid program. This form is specifically designed to streamline the process of requesting medication that may not be readily available or requires special approval. It captures essential patient information, including the patient's name, Medicaid number, and date of birth, ensuring that the request is tied to the correct individual. Additionally, the form requires details from the prescriber, such as their name, license number, and contact information, affirming their commitment to the patient's treatment. The Alabama 390 form also includes sections for the dispensing pharmacy and the specific drug being requested, along with any necessary clinical information and justifications for the request. By providing a clear structure for documenting the rationale behind medication needs, this form helps facilitate timely access to necessary treatments while adhering to Medicaid guidelines. With an emphasis on thorough documentation, the form promotes accountability and ensures that both patients and providers can navigate the complexities of Medicaid pharmacy services with confidence.
| Fact Name | Description |
|---|---|
| Form Purpose | The Alabama 390 form is used to request prior authorization for medications under the Alabama Medicaid program. |
| Governing Law | This form is governed by the Alabama Medicaid Agency regulations, which outline the procedures for medication approval. |
| Patient Information | Essential details about the patient must be provided, including name, Medicaid number, date of birth, and phone number. |
| Prescriber Requirements | The prescriber must include their name, NPI number, and contact information, certifying the necessity of the treatment. |
| Compounding Information | If the request involves compounding, specific ingredients and time units must be detailed on the form. |
| Submission Methods | The completed form can be submitted via fax or mail to the Alabama Medicaid Agency's designated address. |
Filling out the Alabama 390 form requires careful attention to detail to ensure that all necessary information is provided. The form is essential for submitting requests related to Medicaid pharmacy services. Below are the steps to complete the form accurately.
What is the Alabama 390 form?
The Alabama 390 form is a request form used for obtaining prior authorization for pharmacy services under Alabama Medicaid. It is specifically designed for miscellaneous pharmacy requests that require approval before medication can be dispensed.
Who should fill out the Alabama 390 form?
The form should be completed by the prescribing healthcare provider. This includes doctors, nurse practitioners, or any licensed prescriber who is responsible for the patient's treatment.
What information is required on the form?
Essential information includes:
How do I submit the Alabama 390 form?
You can submit the form by faxing it to (800) 748-0116 or mailing it to the address provided on the form: P.O. Box 3210, Auburn, AL 36832-3210.
What happens after I submit the form?
After submission, the Alabama Medicaid Agency will review the request. They may approve, deny, or modify the request based on the information provided. You will receive a response indicating the outcome of your request.
Is there a specific timeframe for approval?
The timeframe for approval can vary. However, it is advisable to submit the form as early as possible to avoid delays in treatment. Generally, a response is provided within a reasonable period after submission.
What if my request is denied?
If your request is denied, you will receive a notification explaining the reasons for the denial. You may have the option to appeal the decision or provide additional information to support your request.
Can I attach additional documentation?
Yes, you can attach additional medical justification or other relevant documents to support your request. Make sure to indicate on the form that you have attached extra documentation.
What is the purpose of the compounding section?
The compounding section is for requests involving customized medications that require specific ingredients. You must list the ingredients and the time required for compounding in this section.
Where can I find more information about the Alabama 390 form?
For more details, you can visit the Alabama Medicaid Agency's website at www.medicaid.alabama.gov. This site provides comprehensive information about the form and the prior authorization process.
Filling out the Alabama 390 form can be a straightforward process, but many individuals make common mistakes that can delay approval or lead to denials. One significant error is failing to provide complete patient information. Omitting essential details such as the patient's Medicaid number or date of birth can result in processing delays. Each section of the form is crucial, and incomplete submissions can lead to unnecessary back-and-forth communication with the Medicaid agency.
Another frequent mistake is neglecting to include the prescriber’s information accurately. The prescriber’s name, NPI number, and contact details must be filled out correctly. If any of this information is incorrect or missing, it can hinder the approval process. The prescriber’s signature is also vital; without it, the request may be deemed invalid.
Many applicants also overlook the importance of providing proper drug and clinical information. This section requires specific details about the drug requested, including the NDC number and the quantity needed. Failing to specify the correct drug or not providing adequate medical justification can lead to a denial. Furthermore, the diagnosis codes must be accurate, as they are used to determine the medical necessity of the request.
Compounding requests present additional challenges. Applicants often forget to list all required compounding ingredients or fail to specify the compounding time units requested. Incomplete information in this section can lead to misunderstandings and delays in processing. It is essential to double-check that all ingredients are listed and that the time required for compounding is clearly stated.
Lastly, many individuals do not attach the necessary supporting documentation. If additional medical justification or EPSDT referral forms are required, they must be included with the submission. Failing to provide this documentation can result in a denial or a request for further information, prolonging the process. Thoroughly reviewing the form and ensuring all sections are complete can significantly improve the chances of approval.
The Alabama 390 form is a crucial document used for requesting prior authorization for certain pharmacy services under Medicaid. However, there are several other forms and documents that often accompany the Alabama 390 form to ensure a smooth and efficient processing of requests. Below is a list of these documents, each serving a specific purpose in the Medicaid process.
Understanding these documents and their roles can help streamline the prior authorization process for Medicaid services. By ensuring that all necessary paperwork is completed and submitted, patients can receive timely access to the medications and treatments they need.
The Alabama 390 form is a request form used for pharmacy prior authorization in the Medicaid system. Several other documents serve similar purposes in healthcare and insurance. Here are seven documents that share similarities with the Alabama 390 form:
When filling out the Alabama 390 form, it is essential to ensure accuracy and completeness. The following list outlines important actions to take and avoid during this process.
Understanding the Alabama 390 form is crucial for both healthcare providers and patients. However, several misconceptions can lead to confusion. Here are nine common misconceptions about the form:
Being aware of these misconceptions can help streamline the process and ensure that patients receive the necessary medications in a timely manner.
When utilizing the Alabama 390 form, it is essential to ensure that the process is clear and efficient. Here are ten key takeaways to consider:
By following these guidelines, individuals can navigate the process of filling out and using the Alabama 390 form more effectively, ultimately ensuring that patients receive the necessary medications in a timely manner.