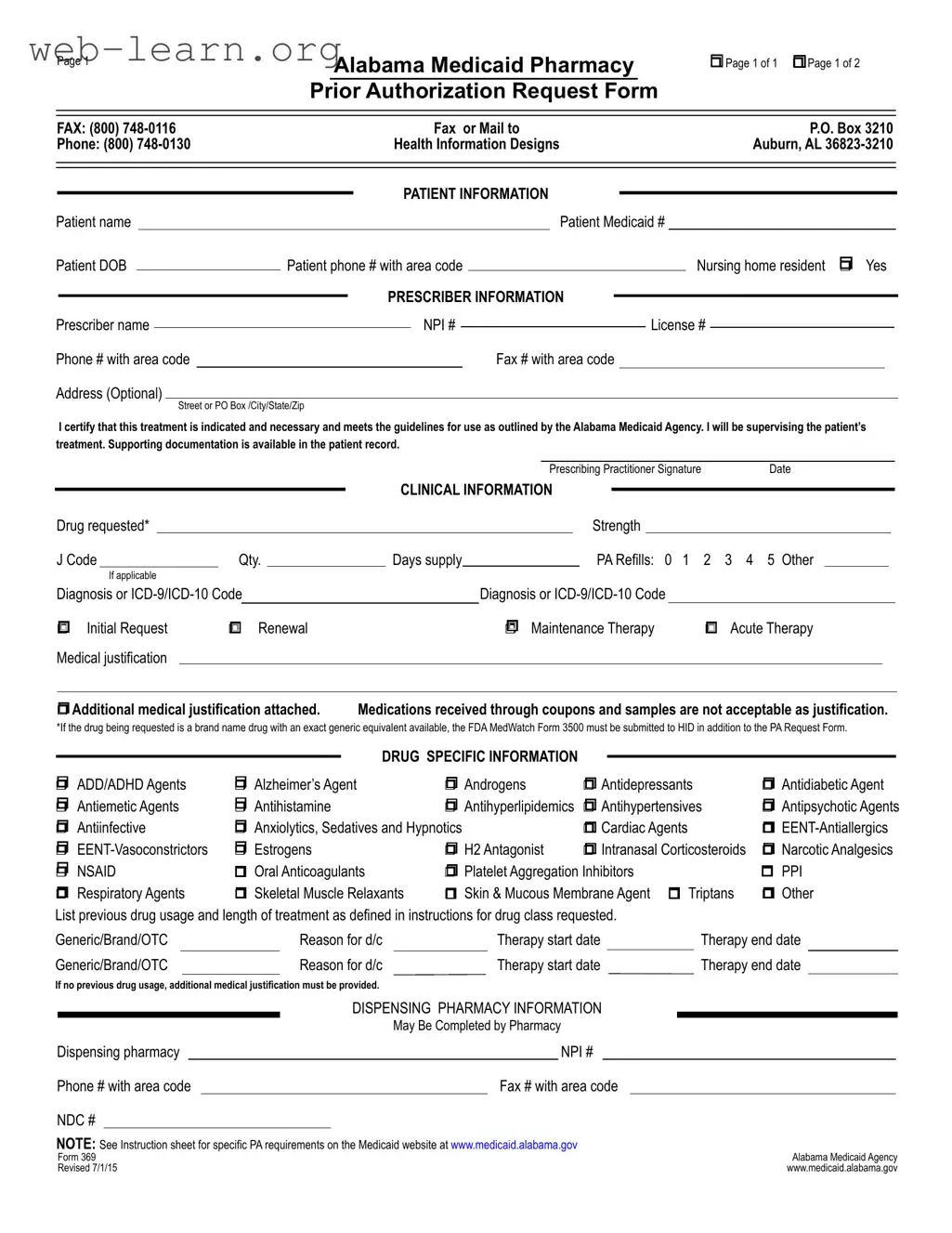
In the realm of healthcare, ensuring that patients receive the medications they need is a top priority. The Alabama 369 form plays a crucial role in this process by serving as the official request for prior authorization of pharmacy services under the Alabama Medicaid program. This form is designed to streamline the approval process for specific medications, ensuring that they align with established medical guidelines. It captures essential patient and prescriber information, including the patient's Medicaid number, date of birth, and contact details, as well as the prescriber's credentials. The form also delves into clinical specifics, such as the requested drug, its strength, and the diagnosis codes that justify the need for the medication. Additionally, it allows for the submission of supporting documentation, which is vital for the approval of both initial requests and renewals. By requiring detailed information about previous therapies and the rationale for the requested treatment, the Alabama 369 form helps to ensure that patients receive appropriate and effective care while maintaining compliance with Medicaid regulations.

| Fact Name | Details |
|---|---|
| Form Purpose | The Alabama 369 form is used to request prior authorization for medications under the Alabama Medicaid program. |
| Governing Law | This form operates under the regulations set by the Alabama Medicaid Agency. |
| Patient Information | Key patient details such as name, Medicaid number, date of birth, and contact information are required. |
| Prescriber Information | Prescribers must provide their name, NPI number, license number, and contact details. |
| Clinical Information | Details about the requested drug, including strength, quantity, and diagnosis codes, must be included. |
| Types of Requests | Requests can be categorized as initial, renewal, or maintenance therapy. |
| Drug Specific Information | The form includes sections for various drug categories, such as antidepressants and antihypertensives. |
| Documentation Requirement | Supporting medical justification must be provided, especially for drugs with no previous usage. |
| Pharmacy Information | Pharmacy details, including NPI number and contact information, may be filled out by the dispensing pharmacy. |
| Submission Method | The completed form can be faxed or mailed to the Alabama Medicaid Agency for processing. |
Filling out the Alabama 369 form is an essential step in the process of obtaining prior authorization for pharmacy services. After completing the form, it should be faxed or mailed to the appropriate address provided on the form. Ensure all required fields are filled accurately to avoid delays in processing.
The Alabama 369 form is a Medicaid Pharmacy Prior Authorization Request Form. It is used by healthcare providers to request prior authorization for specific medications that are covered under Alabama Medicaid. This form ensures that the requested treatment is necessary and meets the guidelines set by the Alabama Medicaid Agency.
The form can be submitted by licensed prescribers who are enrolled in the Alabama Medicaid program. This includes physicians, nurse practitioners, and other qualified healthcare professionals. The prescriber must provide their information, including their name, NPI number, and contact details, as well as the patient's information.
The Alabama 369 form requires detailed information, including:
Completing the form accurately is crucial to ensure timely processing of the request.
The Alabama 369 form can be submitted via fax or mail. To fax the form, send it to (800) 748-0116. Alternatively, it can be mailed to the following address:
P.O. Box 3210
Auburn, AL 36823-3210
For any questions or assistance, prescribers can call (800) 748-0130 for support.
Filling out the Alabama 369 form can be straightforward, but many people make common mistakes that can delay the approval process. One frequent error is neglecting to provide complete patient information. Missing details such as the patient's Medicaid number or date of birth can lead to unnecessary back-and-forth communication with the Medicaid office.
Another mistake is failing to specify the drug requested. The form requires the exact name and strength of the medication. Omitting this information can result in a denial of the request, as the Medicaid agency needs clear details to process the authorization.
Incorrect coding is also a prevalent issue. Many applicants misuse the ICD-9 or ICD-10 codes when indicating the diagnosis. This can cause confusion and may lead to the form being rejected. It is crucial to ensure that the codes align with the patient's medical condition.
Additionally, some people forget to check the appropriate boxes for the type of request. Whether it’s an initial request, renewal, or maintenance therapy, selecting the wrong option can complicate the approval process. Always double-check these selections before submitting the form.
Another common oversight is the lack of medical justification. If the request is for a drug that requires additional documentation, failing to attach this can lead to delays. Ensure that all necessary medical records or justifications are included with the submission.
Furthermore, many applicants overlook the section regarding previous drug usage. If a patient has not used any prior medications, it is essential to provide additional medical justification. Not doing so can result in the request being denied.
Incomplete pharmacy information can also hinder the process. Providing the pharmacy's NPI number and contact information is vital. Missing this information can lead to delays in processing the request.
Some individuals mistakenly believe that medications received through coupons or samples can serve as justification. This is incorrect. The Alabama Medicaid Agency does not accept these as valid medical justification for prior authorization requests.
Finally, failing to sign and date the form is a critical mistake. Without the prescriber’s signature, the request will not be processed. Always ensure that the form is signed and dated before submission to avoid unnecessary delays.
The Alabama 369 form is a crucial document used for requesting prior authorization for pharmacy services under the Alabama Medicaid program. Alongside this form, several other documents are commonly utilized to support the authorization process. Below is a list of these documents, each serving a specific purpose in facilitating patient care and ensuring compliance with Medicaid guidelines.
Each of these documents plays a vital role in the prior authorization process, ensuring that patients receive the necessary medications while adhering to Medicaid regulations. Properly completing and submitting these forms can significantly impact the approval of medication requests.
The Alabama 369 form serves as a Pharmacy Prior Authorization Request for Medicaid patients in Alabama. It plays a crucial role in ensuring that prescribed medications meet specific criteria before they are dispensed. Several other documents share similarities with the Alabama 369 form, primarily in their purpose of obtaining prior authorization for medical services or medications. Below is a list of six documents that are akin to the Alabama 369 form, along with an explanation of how they relate to it.
Understanding these documents can help patients and healthcare providers navigate the often complex process of obtaining necessary medications and services through insurance and Medicaid programs.
When filling out the Alabama 369 form, it's crucial to follow guidelines to ensure a smooth process. Here’s a list of things to do and avoid:
Following these guidelines will help ensure your request is processed efficiently. Double-check your entries for accuracy and completeness before submission.
Understanding the Alabama 369 form is essential for healthcare providers and patients alike. However, several misconceptions can lead to confusion. Here’s a list of common misunderstandings:
Clearing up these misconceptions can help streamline the process for everyone involved. Understanding the correct procedures ensures that patients receive the medications they need in a timely manner.
Here are some important points to remember when filling out and using the Alabama 369 form:
By following these guidelines, you can help ensure that the Alabama 369 form is filled out correctly and efficiently. This will facilitate a smoother approval process for the requested medication.