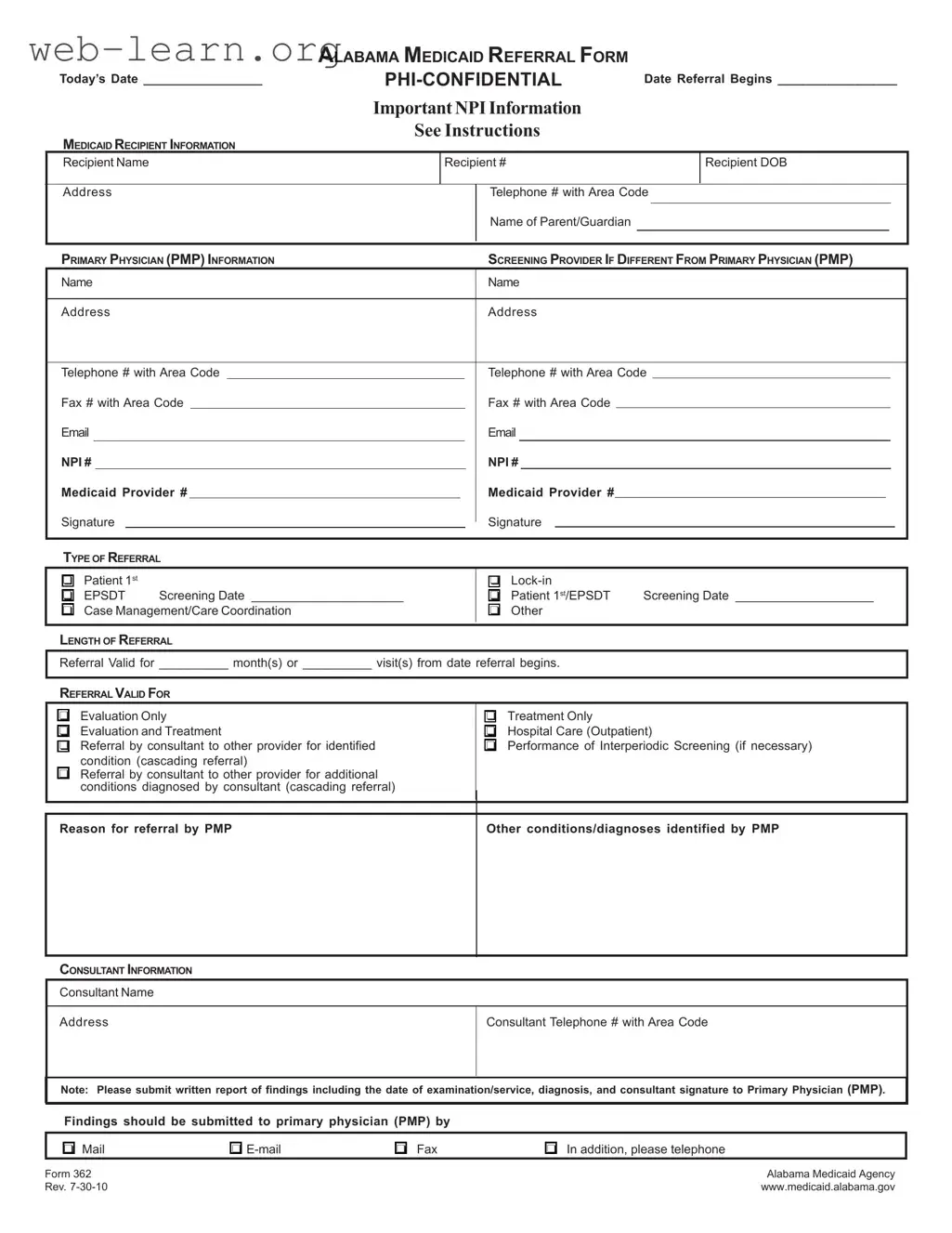
The Alabama 362 form serves as a crucial document in the Medicaid referral process, ensuring that recipients receive the appropriate care they need. This form captures essential details about the Medicaid recipient, including their name, date of birth, and contact information, along with the necessary identifiers like the recipient number. It also gathers information about the primary physician and any other screening providers involved in the patient's care. The form outlines the type of referral being made, whether it is for evaluation, treatment, or case management, and specifies the duration of the referral. Additionally, it provides space for the consultant's information, ensuring that communication between healthcare providers remains streamlined. By requiring signatures from both the primary physician and the consultant, the form emphasizes accountability and collaboration in patient care. Understanding how to correctly fill out and utilize the Alabama 362 form is essential for both healthcare providers and patients navigating the Medicaid system.
| Fact Name | Details |
|---|---|
| Form Purpose | The Alabama 362 form is used for Medicaid referrals, facilitating communication between healthcare providers. |
| Governing Law | This form is governed by Alabama Medicaid regulations and policies. |
| Confidentiality | PHI (Protected Health Information) is marked as confidential on the form, ensuring patient privacy. |
| Recipient Information | Essential details such as the recipient's name, Medicaid number, and date of birth must be provided. |
| Primary Physician Information | Information about the primary physician, including their NPI and Medicaid provider number, is required. |
| Type of Referral | Referrals can be categorized as Patient 1st, EPSDT Screening, or Case Management, among others. |
| Length of Referral | The form allows providers to specify the duration of the referral, either by months or visits. |
| Consultant Information | Details about the consultant, including name and contact information, must be included for follow-up. |
| Submission Instructions | Providers are instructed to submit findings to the primary physician via mail, email, or fax. |
Filling out the Alabama 362 form is an important step in the referral process for Medicaid recipients. Once you complete the form, it will need to be submitted to the appropriate parties for processing. Follow these steps to ensure that you fill out the form correctly.
After completing these steps, review the form for any errors before submission. Ensure that all required information is filled out clearly to avoid delays in processing. Once everything is checked, send the form to the appropriate Medicaid office or provider as needed.
What is the Alabama 362 form?
The Alabama 362 form, also known as the Alabama Medicaid Referral Form, is a document used to refer Medicaid recipients for various medical services. It captures essential information about the patient, their primary physician, and any consultants involved in the patient's care. This form ensures that all necessary details are communicated effectively between healthcare providers.
Who needs to fill out the Alabama 362 form?
The form is typically completed by the primary physician (PMP) of the Medicaid recipient. This physician is responsible for initiating the referral process. Additionally, if there is a screening provider different from the primary physician, they may also need to provide their information on the form.
What information is required on the form?
The Alabama 362 form requires several key pieces of information, including:
What types of referrals can be made using this form?
The Alabama 362 form allows for various types of referrals, including:
How long is a referral valid?
The length of the referral is specified on the form. It can be valid for a certain number of months or a specific number of visits, starting from the date the referral begins. It is important to clearly indicate this duration to avoid any confusion regarding the referral's validity.
What should be done after the consultation?
After the consultation, the consultant is required to submit a written report of their findings. This report should include the date of examination, diagnosis, and the consultant's signature. The findings must be sent to the primary physician, either by mail, email, fax, or another agreed-upon method.
Can the form be used for multiple conditions?
Yes, the Alabama 362 form can accommodate referrals for multiple conditions. If a consultant identifies additional conditions during their evaluation, these can be documented on the form under the appropriate sections. This allows for comprehensive care coordination.
Where can I find more information about the form?
Additional details about the Alabama 362 form can be found on the Alabama Medicaid Agency's official website. This resource provides guidance on completing the form and offers updates on any changes to the referral process.
What happens if the form is not filled out correctly?
If the Alabama 362 form is not completed accurately, it may lead to delays in care or complications with Medicaid billing. It is essential to ensure that all information is correct and complete before submission. Inaccuracies can hinder the referral process and affect the recipient's access to necessary services.
Filling out the Alabama 362 form can be straightforward, but mistakes can lead to delays in processing or even denial of services. One common error is failing to include the Medicaid Recipient Information completely. This section requires accurate details such as the recipient's name, number, date of birth, address, and telephone number. Omitting any of this information can result in significant delays.
Another frequent mistake is not providing the correct Primary Physician (PMP) Information. The form requires the name, address, and contact details of the primary physician. If this information is incorrect or missing, it may hinder communication between providers and affect the recipient's care.
Many individuals also overlook the importance of specifying the Type of Referral. This section has multiple options, and selecting the wrong one can lead to confusion about the purpose of the referral. It is essential to carefully review the options and choose the one that accurately reflects the situation.
Additionally, some people fail to indicate the Length of Referral properly. This section asks for either the number of months or visits for which the referral is valid. Not providing this information can result in the referral being deemed invalid.
When it comes to the Consultant Information, errors often occur. This includes providing incorrect contact details for the consultant. If the consultant's name, address, or phone number is wrong, it can complicate the process of obtaining necessary evaluations or treatments.
Another mistake is neglecting to sign the form. The Signature section is critical, and failing to sign can lead to the form being rejected outright. It is essential to ensure that all required signatures are present before submission.
Some individuals also forget to specify the Reason for Referral. This detail is crucial for the receiving provider to understand the context of the referral. Without a clear reason, the referral may not be processed as intended.
In addition, many people do not submit the required written report of findings from the consultant. This report is necessary for the primary physician to understand the outcomes of the consultation. Failing to include this report can delay further treatment.
Lastly, using outdated or incorrect versions of the form can lead to complications. Always ensure that the most current version of the Alabama 362 form is being used to avoid any issues with compliance or processing.
The Alabama 362 form is a crucial document used for Medicaid referrals in Alabama. It captures essential information about the recipient, the primary physician, and the details of the referral. Alongside this form, several other documents are often utilized to ensure a smooth referral process. Below is a list of these commonly used forms and documents.
Each of these documents plays a significant role in the Medicaid referral process. Together, they help ensure that recipients receive the appropriate care while maintaining compliance with regulations. Understanding these forms can simplify interactions with the healthcare system and enhance the overall experience for both providers and patients.
The Alabama 362 form serves as a crucial document for Medicaid referrals in the state of Alabama. It is not unique in its function; several other forms fulfill similar roles in healthcare and insurance contexts. Below are five documents that share similarities with the Alabama 362 form:
When filling out the Alabama 362 form, it's essential to follow specific guidelines to ensure your submission is accurate and complete. Here’s a list of things you should and shouldn’t do:
By following these tips, you can help ensure a smoother process when using the Alabama 362 form.
Understanding the Alabama 362 form is essential for both healthcare providers and patients. However, several misconceptions can lead to confusion. Here’s a look at nine common misunderstandings about this important document:
By clarifying these misconceptions, both healthcare providers and patients can navigate the referral process more effectively. Understanding the Alabama 362 form helps ensure that necessary care is accessed without unnecessary delays.
When filling out the Alabama 362 form, it's essential to keep a few key points in mind. Here are some important takeaways:
By following these guidelines, you can ensure that the Alabama 362 form is completed correctly and efficiently, facilitating the necessary medical referrals.