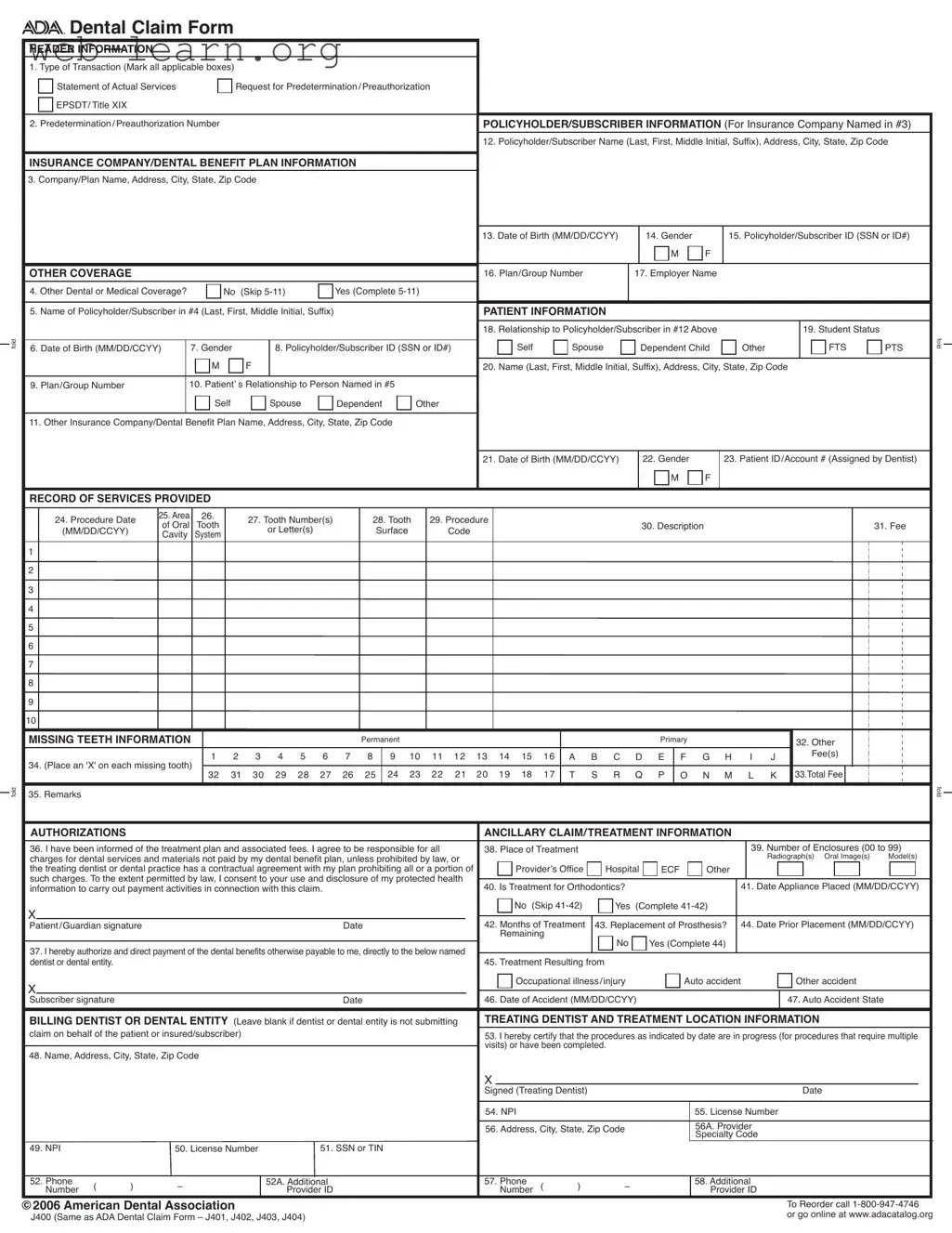
The ADA Dental Claim Form is an essential document for dental professionals seeking reimbursement from insurance companies for services rendered. This form captures vital information about the transaction type, including whether it is a statement of actual services or a request for preauthorization. Key sections include details about the policyholder and subscriber, such as names, addresses, and policy numbers, ensuring that the claim is correctly attributed. Patient information is also crucial, encompassing their relationship to the policyholder, date of birth, and any other insurance coverage that may apply. The record of services provided section outlines specific procedures performed, including dates, tooth numbers, and associated fees. Additionally, the form requires authorizations, confirming that patients understand their treatment plans and financial responsibilities. Dentists must also provide their credentials, including their National Provider Identifier (NPI) and specialty codes, to facilitate accurate processing. Overall, the ADA Dental Claim Form is designed to streamline the claims process, ensuring that all necessary information is submitted for efficient reimbursement.

| Fact Name | Fact Description |
|---|---|
| Form Purpose | The ADA Dental Claim Form is used to submit claims for dental services to insurance companies or dental benefit plans. |
| Transaction Types | Claimants can indicate multiple transaction types on the form, including a statement of actual services and requests for predetermination or preauthorization. |
| Policyholder Information | Essential details about the policyholder, such as name and address, must be provided in the designated sections of the form. |
| Patient Relationship | The form requires the relationship of the patient to the policyholder to be specified, which helps clarify coverage eligibility. |
| Missing Teeth Information | Claimants must indicate any missing teeth by marking the appropriate sections, which is crucial for determining treatment coverage. |
| Authorization Requirement | Patients or guardians must authorize the release of their protected health information for payment activities related to the claim. |
| National Provider Identifier (NPI) | Providers must include their NPI, which is a unique identifier assigned by the federal government to healthcare providers. |
| Coordination of Benefits | If there is secondary insurance, the form must be completed in full, and the primary payer's Explanation of Benefits must be attached. |
| State-Specific Regulations | Each state may have specific laws governing the use of the ADA Dental Claim Form, which should be reviewed for compliance. |
Completing the ADA Dental Claim form is an essential step in submitting a claim for dental services. Following these instructions will help ensure that all necessary information is accurately filled out, facilitating a smoother claims process.
The ADA Dental Claim Form is used to submit claims for dental services to insurance companies or dental benefit plans. It helps ensure that both the provider and the patient receive the appropriate reimbursement for the services rendered. Completing the form accurately is crucial for a smooth claims process.
The form requires several key pieces of information:
Completing all relevant fields is essential to avoid delays in processing.
Once you have completed the ADA Dental Claim Form, you can submit it directly to the insurance company or dental benefit plan. Ensure that the name and address of the payer are visible in a standard #10 envelope. Folding the form at the designated tick marks will help facilitate this process.
If you have other coverage, you must complete the additional sections of the form. This includes providing details about the other policyholder/subscriber and their coverage. Make sure to include any relevant information about the primary payer’s payment, as this will help with coordination of benefits.
If the number of procedures exceeds the available lines on the form, you will need to complete a separate claim form for the additional procedures. Ensure that each form is fully filled out to avoid confusion and ensure all services are accounted for.
The NPI is a unique identifier assigned to healthcare providers by the federal government. It is essential for billing purposes and helps to streamline the claims process. Dentists must include their NPI on the claim form to ensure proper identification and reimbursement.
Incomplete or inaccurate forms can lead to delays in processing claims or even denials. It’s important to double-check all information before submission. If a claim is denied, you may need to resubmit with corrections, which can prolong the reimbursement process.
Filling out the ADA Dental Claim Form can be straightforward, but many people make mistakes that can delay processing or lead to claim denials. One common error is leaving out essential information. Each section of the form must be completed unless specified otherwise. If a required field is left blank, the claim may be returned for correction. Always double-check that all necessary details, such as names, addresses, and dates, are filled in correctly.
Another frequent mistake is not using the correct format for dates. The form requires dates to be entered in the MM/DD/CCYY format. If someone writes a date in a different format, it can lead to confusion and processing delays. Remember, clarity is key. Using the right format helps ensure that the claim is processed smoothly.
Many people also forget to include the National Provider Identifier (NPI) for the dentist. This identifier is crucial for claims processing and helps verify the provider's credentials. If the NPI is missing, the insurance company may not process the claim. Always ensure that the NPI is included and accurate.
Another common issue arises when individuals fail to indicate whether there is other dental or medical coverage. If there is additional coverage, it's vital to complete the relevant sections of the form. Not doing so can result in the claim being denied or delayed. Always check for any additional insurance and provide the necessary details.
Lastly, some individuals neglect to sign the form. A signature is required to authorize the payment of benefits and to confirm that the information provided is accurate. Without a signature, the claim cannot be processed. Ensure that the form is signed and dated before submission to avoid unnecessary delays.
The ADA Dental Claim Form is a crucial document used in the dental field to facilitate the submission of claims to insurance companies. However, it is often accompanied by other forms and documents that help to provide additional information or clarify details regarding the claim. Below is a list of some of these essential documents.
In summary, while the ADA Dental Claim Form is a fundamental part of the claims process, these accompanying documents play a vital role in ensuring that claims are processed efficiently and accurately. Together, they help to streamline communication between dental practices and insurance providers, ultimately benefiting the patient.
The ADA Dental Claim form shares similarities with several other documents commonly used in the healthcare and insurance industries. Below is a list of seven documents that are comparable, highlighting their similarities.
When filling out the ADA Dental Claim form, attention to detail is crucial. Here are some important do's and don'ts to ensure your submission is accurate and complete.
By following these guidelines, you can help ensure that your dental claim is processed smoothly and efficiently. Careful attention to the details not only supports timely reimbursement but also fosters positive communication with your dental provider and insurance company.
This form is versatile and can be used for various transactions, including requests for preauthorization and EPSDT services. It accommodates different types of claims beyond just dental treatments.
While it is important to complete most fields, some may not be required based on the specific situation. Always check the instructions for guidance on which fields can be left blank.
Patients or their guardians can also submit the claim. If the dentist is submitting on behalf of the patient, they will need to fill out specific sections of the form.
Both the policyholder and the patient must have their date of birth included on the form. This information is crucial for identification and processing purposes.
The NPI is essential for all healthcare providers considered HIPAA covered entities. It helps in uniquely identifying providers and streamlining the claims process.
It is important to indicate any missing teeth on the form. This information can impact the coverage and payment for the procedures performed.
While the ADA Dental Claim Form is standardized, some insurance companies may have additional requirements. Always verify with the specific insurance provider to ensure compliance.
If the number of procedures exceeds the lines available on the form, a separate claim form must be completed for the additional procedures. This ensures clarity and accuracy in processing.
When submitting a claim to a secondary payer, it is necessary to attach the primary payer's EOB. This document shows what was covered and how much was paid, which is vital for the secondary claim's processing.
For clarity and accuracy, it is recommended to complete the form using typed or printed information. Handwritten entries can lead to misunderstandings and delays in processing.
Filling out the ADA Dental Claim Form accurately is essential for ensuring timely processing and reimbursement. Here are key takeaways to keep in mind:
By adhering to these guidelines, individuals can facilitate a smoother claims process and minimize potential issues with their dental insurance providers.