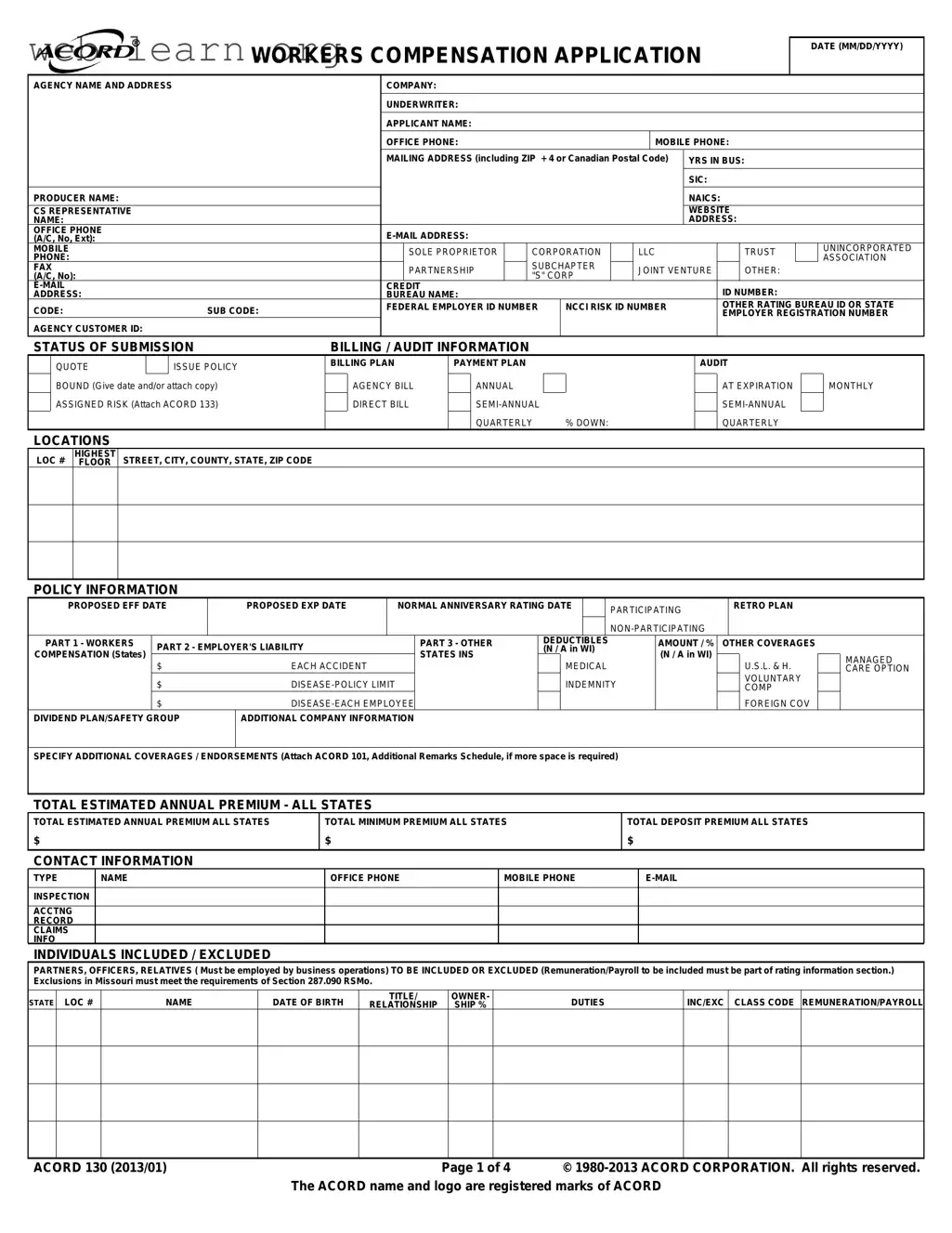
The ACORD 130 form plays a crucial role in the process of obtaining workers' compensation insurance for businesses across the United States. This comprehensive application gathers essential information about the applicant, including their business structure, contact details, and years in operation. It also requires specifics about the nature of the business, including the types of operations and any potential risks associated with them. The form outlines various sections where applicants must provide details regarding their employees, including their classification, payroll estimates, and any exclusions that may apply. Additionally, the ACORD 130 captures prior carrier information and loss history, which is vital for insurers to assess the risk profile of the applicant. With sections dedicated to billing and audit information, as well as coverage options, the form ensures that all necessary details are available for underwriters to make informed decisions. Overall, the ACORD 130 serves as a foundational document that facilitates the underwriting process while helping businesses secure the necessary coverage to protect their employees and operations.
| Fact Name | Detail |
|---|---|
| Form Purpose | The ACORD 130 form is used to apply for workers' compensation insurance. |
| Application Date | Applicants must provide the application date in MM/DD/YYYY format. |
| Contact Information | The form requires detailed contact information for the applicant, including phone numbers and email addresses. |
| Business Structure | Applicants must indicate their business structure, such as corporation, LLC, or sole proprietorship. |
| State-Specific Information | For states like Missouri, specific laws govern the inclusion of exclusions in the application. |
| Estimated Premiums | The form requires estimations for annual premiums, including total estimated and minimum premiums. |
| Loss History | Applicants must provide loss history for the past five years, detailing claims and amounts paid. |
| General Information | Questions regarding hazardous materials, subcontractors, and employee demographics are included. |
| Fraud Warning | The form includes a warning about the consequences of providing false information, which may lead to criminal penalties. |
| Signature Requirement | The application must be signed by an authorized representative, such as an officer or partner of the business. |
Completing the ACORD 130 form is an important step in applying for workers' compensation insurance. This form collects essential information about your business, its operations, and the coverage you seek. By accurately filling it out, you help ensure that your application is processed smoothly and that you receive the appropriate coverage for your needs.
After completing the form, review all entries for accuracy. It's essential to ensure that every section is filled out correctly to avoid delays in processing your application. Once verified, submit the form to your insurance agent or broker for further action.
The ACORD 130 form is primarily used to apply for workers' compensation insurance. It collects essential information about the applicant's business, including details about operations, employee classifications, and previous insurance coverage. This information helps insurance companies assess the risk associated with providing coverage.
Any business that employs workers and seeks workers' compensation insurance must complete the ACORD 130 form. This includes various business structures such as sole proprietorships, corporations, limited liability companies (LLCs), and partnerships. Regardless of the business type, accurate information is crucial for obtaining appropriate coverage.
The form requests a variety of information, including:
Providing complete and accurate information is essential for processing the application effectively.
If you have had previous claims, it is important to disclose this information on the ACORD 130 form. The form includes a section for loss history, where you can provide details about past claims, including the amount paid and reserves. Transparency in this area can help in obtaining fair premium rates.
The information provided on the ACORD 130 form directly impacts the calculation of your insurance premium. Factors such as the type of business, employee classifications, and previous claims history will be considered by the insurer. Accurate reporting of payroll and employee duties can lead to more accurate premium assessments.
Once the ACORD 130 form is submitted, any necessary changes should be communicated to your insurance agent or broker as soon as possible. They can assist in making amendments to the application or provide guidance on how to proceed if new information arises.
After submission, the insurance company will review the information provided on the ACORD 130 form. They may contact you for additional information or clarification. Once the review is complete, you will receive a quote for your workers' compensation coverage, which you can then accept or decline.
Filling out the ACORD 130 form can be a straightforward process, but many people make common mistakes that can lead to delays or complications. One major mistake is failing to provide complete contact information. This includes not listing the correct agency name, address, and phone numbers. Incomplete contact details can hinder communication and slow down the application process.
Another frequent error is neglecting to specify the type of business entity. Whether it’s a corporation, LLC, or sole proprietorship, accurately identifying the business type is crucial. Incorrect designations can result in inappropriate coverage or premium calculations.
Many applicants also overlook the importance of listing all employees accurately. It’s essential to include both full-time and part-time employees, along with their roles and remuneration. Missing or incorrect employee details can lead to miscalculations in the estimated annual premium.
Additionally, some people fail to provide the correct Federal Employer Identification Number (FEIN). This number is vital for tax purposes and helps in identifying the business. Omitting or misentering this number can cause significant issues with the application.
Another common mistake is not attaching necessary documents, such as loss runs or additional remarks. These documents provide critical context and information that insurers need to assess risk accurately. Without them, the application may be incomplete.
Inaccurate or incomplete information regarding prior insurance coverage is also a common issue. Applicants should provide details about any past claims or coverage, as this history can affect current premiums and eligibility.
Failing to explain “yes” responses in the general information section can lead to misunderstandings. If any questions are answered affirmatively, it’s essential to provide detailed explanations to avoid confusion later.
People often forget to sign the application. An unsigned form is not valid and will be rejected. Ensure that the authorized representative signs and dates the application before submission.
Lastly, many applicants do not double-check for errors or omissions before submitting the form. A thorough review can catch mistakes that could delay processing or lead to coverage issues. Taking the time to verify all information can save headaches down the line.
The ACORD 130 form is an essential document used in the application process for workers' compensation insurance. Alongside this form, several other documents may be required to provide a comprehensive overview of the applicant's business operations and risk factors. Below is a list of commonly used forms and documents that accompany the ACORD 130 form, along with a brief description of each.
Each of these documents plays a vital role in the overall evaluation process for workers' compensation insurance. Providing complete and accurate information in conjunction with the ACORD 130 form can significantly facilitate the underwriting process and ensure that the applicant receives the appropriate coverage for their needs.
When filling out the ACORD 130 form, attention to detail is crucial. Here are some important dos and don’ts to consider:
This form is applicable to businesses of all sizes, including small and medium enterprises. Regardless of the scale, if a business requires workers' compensation insurance, it must complete this form.
Filling out the form does not automatically ensure that coverage will be granted. The insurance company will review the information and determine eligibility based on various factors.
It is essential to include all relevant individuals, such as partners, officers, and employees, especially those who may be included or excluded from coverage.
While it is a critical document, additional forms or information may be required, depending on the specific circumstances of the business and state regulations.
Variations exist in the Acord 130 form depending on state requirements. It is crucial to ensure that the correct version for your state is used.
Any significant changes in the business, such as ownership or operational scope, should prompt an update to the information on the form to ensure accuracy and compliance.
Providing a complete loss history for the past five years is often necessary. This information helps insurers assess risk and determine premiums.
Leaving sections blank can lead to delays or complications in the application process. It is best to provide as much information as possible or indicate if something is not applicable.
Established businesses must also complete this form during policy renewals or when changing insurance providers. It remains relevant throughout the life of the business.