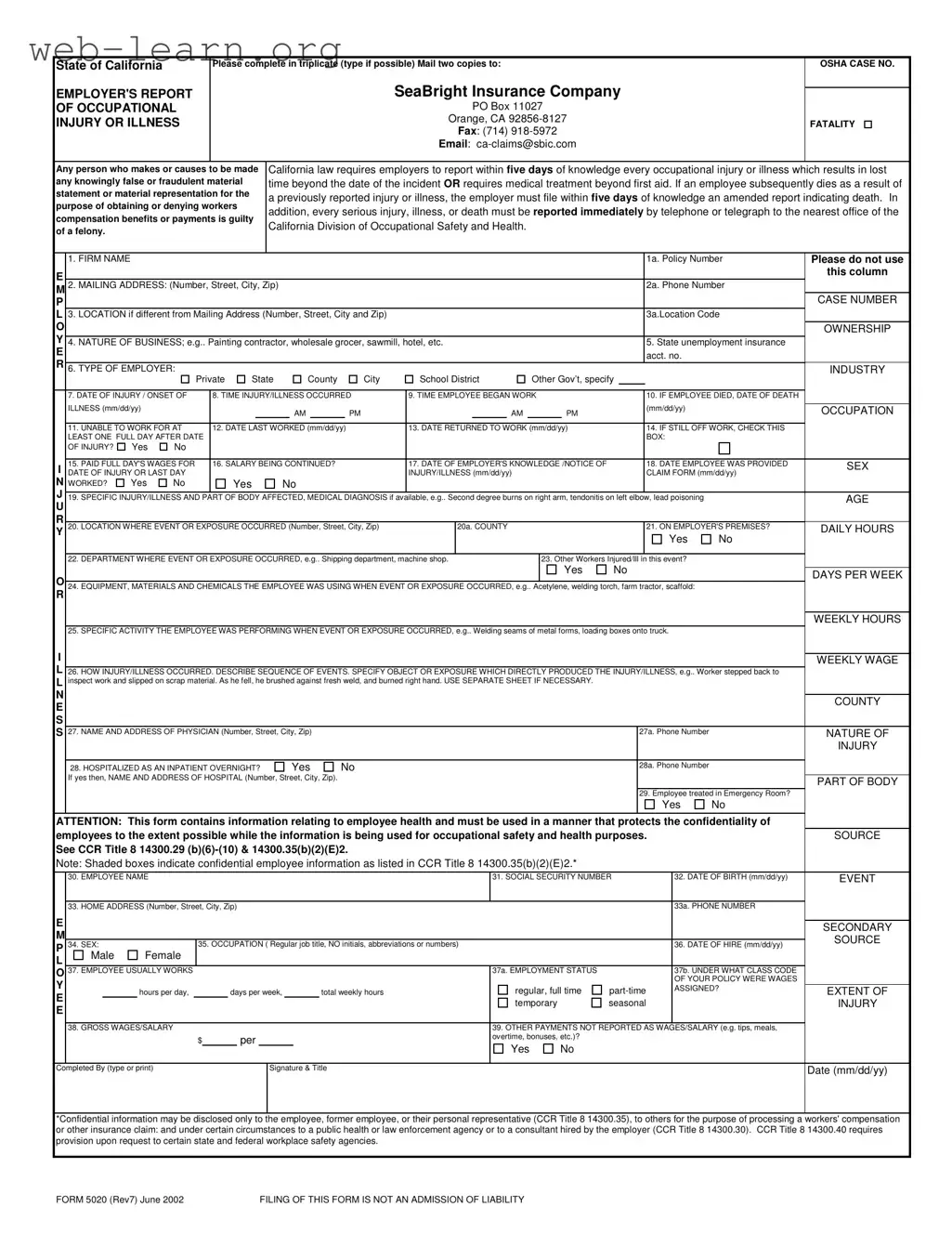
The 5020 California form is a critical document for employers reporting occupational injuries or illnesses. This form must be completed in triplicate and submitted to SeaBright Insurance Company within five days of the employer's knowledge of an incident that results in lost work time or requires medical treatment beyond first aid. It serves as an official record that not only tracks injuries but also ensures compliance with state regulations. Employers must provide detailed information, including the nature of the injury, the circumstances surrounding it, and the employee's work status. If an employee dies due to a reported injury, an amended report is required within five days. Additionally, serious injuries must be reported immediately to the California Division of Occupational Safety and Health. The form captures essential details such as the employee's personal information, the specifics of the injury, and the employer's knowledge of the incident. By adhering to these reporting requirements, employers help maintain workplace safety and ensure that employees receive the necessary care and benefits.
| Fact Name | Description |
|---|---|
| Purpose | The 5020 California form is used by employers to report occupational injuries or illnesses. |
| Submission Requirements | Employers must complete the form in triplicate and send two copies to SeaBright Insurance Company. |
| Reporting Timeframe | California law mandates that injuries resulting in lost time or requiring medical treatment be reported within five days of knowledge. |
| Amended Reports | If an employee dies from a previously reported injury, an amended report must be filed within five days of knowledge of the death. |
| Immediate Reporting | Serious injuries or deaths must be reported immediately to the California Division of Occupational Safety and Health. |
| Confidentiality | The form contains confidential employee information and must be handled accordingly to protect privacy. |
| Legal Consequences | Filing false information on the form is a felony under California law. |
| Governing Laws | This form is governed by California Code of Regulations (CCR) Title 8, Sections 14300.29 and 14300.35. |
Completing the 5020 California form is an important step for employers when reporting occupational injuries or illnesses. This process ensures that necessary information is documented and submitted to the appropriate parties. After filling out the form, you will need to mail two copies to SeaBright Insurance Company and keep one for your records. Below are the steps to help you fill out the form accurately.
What is the purpose of the 5020 California form?
The 5020 California form is designed for employers to report occupational injuries or illnesses that occur in the workplace. This includes incidents that result in lost time beyond the date of the incident or require medical treatment beyond first aid. The form must be completed in triplicate and submitted to the designated insurance company.
Who is required to fill out the 5020 form?
Employers in California are required to complete the 5020 form whenever an employee experiences a work-related injury or illness that meets the reporting criteria. This includes private employers, state agencies, and various governmental entities.
What information must be provided on the form?
The form requires several pieces of information, including:
When must the 5020 form be submitted?
The form must be submitted within five days of the employer's knowledge of the injury or illness. If the employee dies as a result of the incident, an amended report must be filed within five days of that knowledge.
How should the form be submitted?
Employers must complete the form in triplicate. Two copies should be mailed to SeaBright Insurance Company at the specified address. Additionally, employers can also send the form via fax or email as provided on the form.
What happens if false information is provided on the form?
Providing false or fraudulent information on the 5020 form is considered a felony under California law. This applies to anyone who knowingly makes false statements to obtain or deny workers' compensation benefits.
Is there any confidential information on the form?
Yes, the form contains confidential employee information, such as social security numbers and medical details. Employers must handle this information with care and ensure it is used only for occupational safety and health purposes.
What should an employer do if multiple employees are injured in the same incident?
If more than one employee is injured, the employer must report each injury individually on separate forms. This ensures that all incidents are documented accurately and appropriately for workers' compensation purposes.
Filling out the 5020 California form accurately is crucial for ensuring that occupational injuries or illnesses are reported correctly. However, many people make mistakes that can lead to delays or complications in processing claims. One common error is failing to provide complete information in the FIRM NAME and MAILING ADDRESS sections. Omitting details such as the complete address or policy number can create confusion and hinder communication with the insurance company.
Another frequent mistake involves the DATE OF INJURY and TIME INJURY/ILLNESS OCCURRED fields. It’s vital to enter the correct dates and times, as inaccuracies can affect the validity of the report. If the date of injury is not clearly documented, it may lead to disputes regarding the claim. Additionally, ensure that the time is noted in the correct format, as this can also complicate matters.
People often overlook the importance of detailing the SPECIFIC INJURY/ILLNESS AND PART OF BODY AFFECTED. Providing vague descriptions can lead to misunderstandings about the nature of the injury. It is essential to be as specific as possible, including medical diagnoses if available. This information is critical for both the employer’s records and the insurance company’s assessment of the claim.
Lastly, failing to indicate whether the employee was hospitalized or treated in an emergency room is a significant oversight. The HOSPITALIZED AS AN INPATIENT OVERNIGHT? and Employee treated in Emergency Room? questions must be answered accurately. This information helps the insurance company understand the severity of the injury and can impact the claim’s outcome. Ensuring that all sections of the form are completed with accurate and detailed information is essential for a smooth claims process.
The 5020 California form is a critical document for employers reporting occupational injuries or illnesses. In addition to this form, several other documents are often required or beneficial in the claims process. Below is a list of these documents, each serving a specific purpose in ensuring compliance and facilitating communication between employers, employees, and insurance companies.
Understanding these additional forms and their purposes can streamline the claims process and ensure compliance with California's workers' compensation regulations. Proper documentation is essential for both employers and employees to navigate the complexities of occupational injury reporting and claims management effectively.
When filling out the 5020 California form, it is essential to follow certain guidelines to ensure accuracy and compliance. Below is a list of things to do and avoid.
Understanding the 5020 California form is essential for employers. However, several misconceptions can lead to confusion. Here are seven common misunderstandings:
Being aware of these misconceptions can help ensure compliance and protect both employers and employees. Properly understanding the requirements of the 5020 form is crucial for maintaining workplace safety and meeting legal obligations.
Filling out and using the 5020 California form is crucial for employers reporting occupational injuries or illnesses. Here are some key takeaways to keep in mind:
By following these guidelines, employers can ensure compliance with California law and contribute to a safer workplace.